In order to be exempt from Ohio income tax, taxpayers need to complete and submit Form Doh 4291A. This form is used to certify that the taxpayer meets the conditions for exemption and to claim the exemption amount. The deadline for filing this form is May 1st of the year following the tax year for which the exemption is claimed. There are a few things taxpayers should keep in mind when completing Form Doh 4291A, including what documentation is required to support their claim. In this blog post, we will provide an overview of what you need to know about Form Doh 4291A so you can successfully file it on time. Stay tuned for more information!
| Question | Answer |
|---|---|
| Form Name | Doh 4291A Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | agent application form template, online agent application, agent registration form pdf, agent recruitment form |
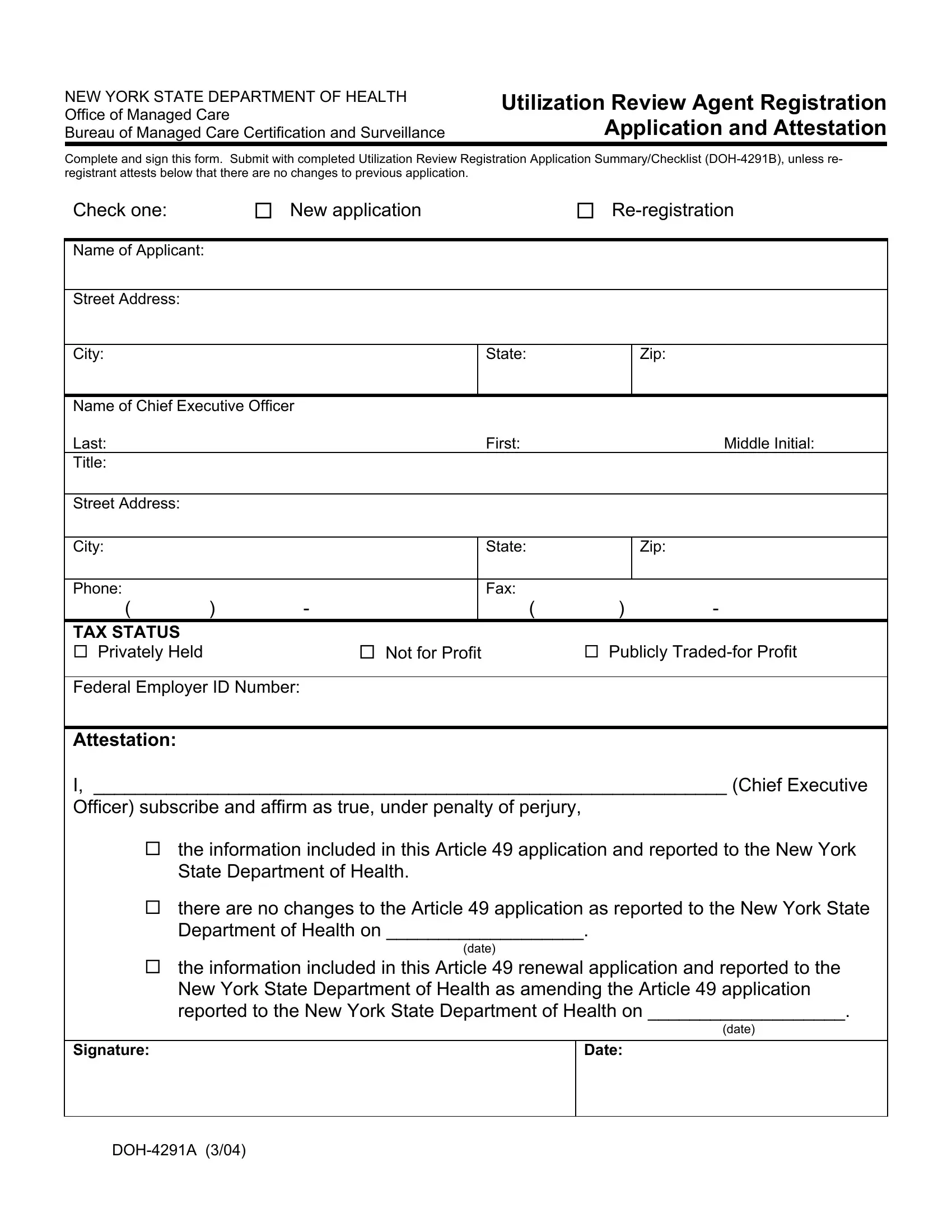
NEW YORK STATE DEPARTMENT OF HEALTH Office of Managed Care
Bureau of Managed Care Certification and Surveillance
Utilization Review Agent Registration Application and Attestation
Complete and sign this form. Submit with completed Utilization Review Registration Application Summary/Checklist
Check one: |
New application |
Name of Applicant:
Street Address:
City:
State:
Zip:
Name of Chief Executive Officer |
|
|
|
|
|
|
Last: |
|
|
|
First: |
|
Middle Initial: |
Title: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
State: |
|
Zip: |
|
|
|
|
|
|
|
Phone: |
|
|
|
Fax: |
|
|
( |
) |
- |
|
( |
) |
- |
TAX STATUS |
|
|
|
|
|
|
Privately Held |
|
|
Not for Profit |
Publicly |
||
Federal Employer ID Number:
Attestation:
I, _____________________________________________________________ (Chief Executive
Officer) subscribe and affirm as true, under penalty of perjury,
the information included in this Article 49 application and reported to the New York State Department of Health.
there are no changes to the Article 49 application as reported to the New York State Department of Health on ___________________.
(date)
the information included in this Article 49 renewal application and reported to the New York State Department of Health as amending the Article 49 application reported to the New York State Department of Health on ___________________.
(date)
Signature:
Date: