

DOH 4329 Form can be filled in online very easily. Simply try FormsPal PDF tool to complete the job quickly. In order to make our editor better and less complicated to work with, we constantly implement new features, with our users' suggestions in mind. By taking a few easy steps, you may start your PDF journey:
Step 1: Click on the "Get Form" button above on this webpage to get into our PDF tool.
Step 2: This editor will let you customize your PDF in a range of ways. Improve it by writing personalized text, correct existing content, and place in a signature - all when it's needed!
Filling out this form needs care for details. Ensure all necessary blanks are filled out properly.
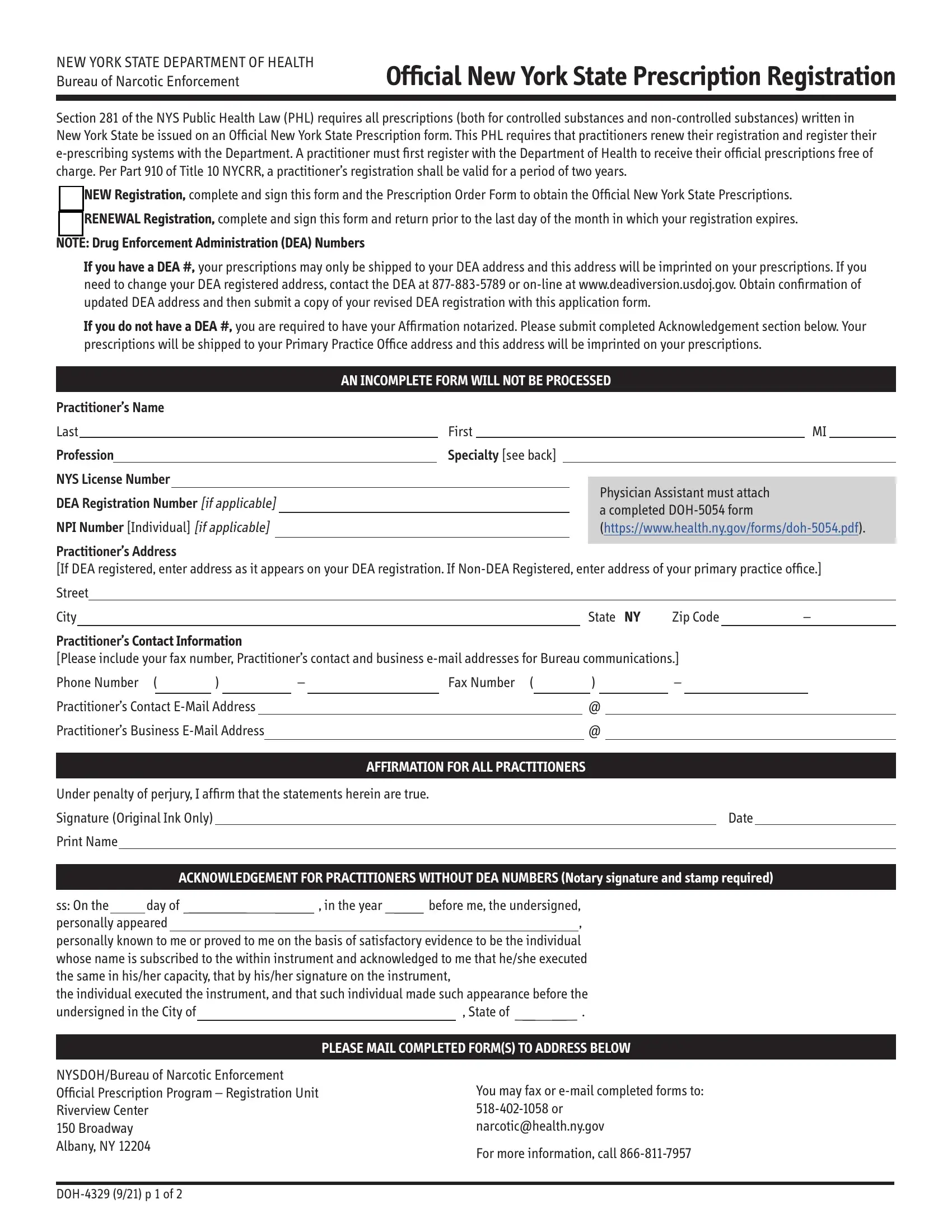
1. You will want to fill out the DOH 4329 Form accurately, thus be attentive when working with the segments including all of these blank fields:
2. Soon after this section is filled out, go on to type in the relevant details in these: Practitioners Contact Information, Phone Number, Fax Number, Practitioners Contact EMail Address, Practitioners Business EMail, AFFIRMATION FOR ALL PRACTITIONERS, Under penalty of perjury I affirm, Signature Original Ink Only, Print Name, Date, ACKNOWLEDGEMENT FOR PRACTITIONERS, ss On the day of in the year, PLEASE MAIL COMPLETED FORMS TO, and NYSDOHBureau of Narcotic.
You can certainly get it wrong while completing the NYSDOHBureau of Narcotic, so make sure to take another look before you decide to send it in.
Step 3: Just after proofreading your filled in blanks, press "Done" and you're all set! Sign up with FormsPal today and easily gain access to DOH 4329 Form, available for download. All modifications you make are saved , which enables you to edit the pdf later when necessary. FormsPal guarantees your information confidentiality via a secure method that never records or shares any sort of personal information provided. Be confident knowing your files are kept protected every time you use our editor!