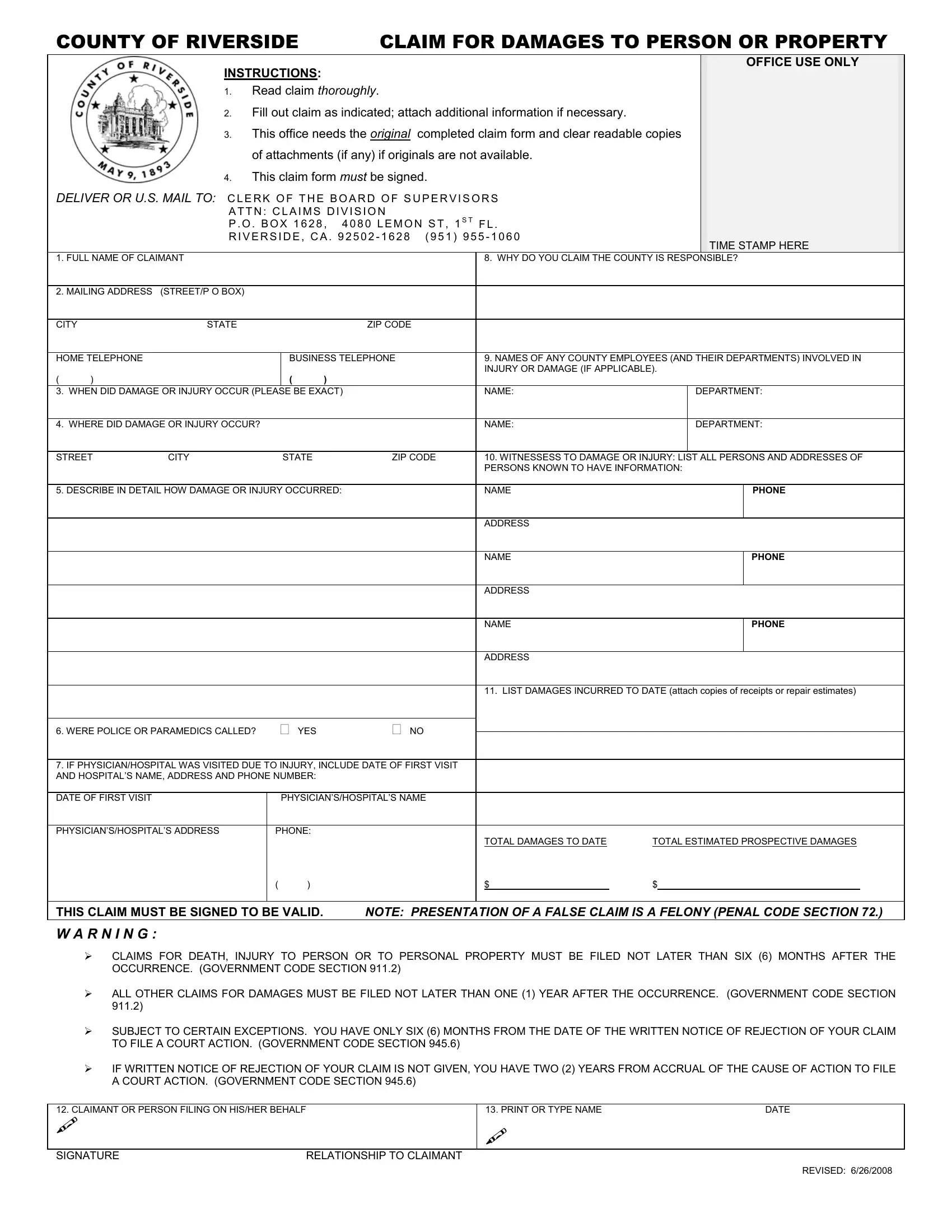
In the intricate web of procedures that victims of domestic violence must navigate, the Domestic Violence Claim Form for Riverside County stands as a critical document for those seeking justice and compensation for their injuries or damage to property. This comprehensive form, designed for submission to the Riverside County Clerk of the Board of Supervisors, requires meticulous attention to detail, starting from reading the claim thoroughly to providing a detailed account of the incident, including the exact date, location, and how the damage or injury occurred. Key aspects include identifying any county employees involved, listing witnesses, and quantifying damages incurred, supported by receipts or repair estimates. It emphasizes the necessity of a timely submission, with strict deadlines for filing claims related to personal injury, death, or property damage. The claim must be signed to be considered valid, and it comes with stern warnings against the presentation of false claims—a felony under the Penal Code Section 72. Additionally, it outlines the urgent timelines for legal action following the rejection of a claim, underscoring the importance of understanding one's rights and the potential consequences of missing critical deadlines. This form not only serves as a vehicle for pursuing claims but also as a reminder of the legal frameworks designed to hold responsible parties accountable and provide a pathway for victims to seek reparations.
| Question | Answer |
|---|---|
| Form Name | Domestic Violence Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | riverside claim form, riverside county forms online, riverside county civil forms, claim damages person form |
COUNTY OF RIVERSIDE |
|
CLAIM FOR DAMAGES TO PERSON OR PROPERTY |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSTRUCTIONS: |
|
|
|
|
|
|
|
|
OFFICE USE ONLY |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
1. |
Read claim thoroughly. |
|
|
|
|
|
|
|
|
||||
|
|
2. |
Fill out claim as indicated; attach additional information if necessary. |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||||||
|
|
3. |
This office needs the original |
completed claim form and clear readable copies |
|
|
|
|
|||||||
|
|
|
of attachments (if any) if originals are not available. |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
4. |
This claim form must be signed. |
|
|
|
|
|
|
|
|||||
DELIVER OR U.S. MAIL TO: CLERK OF THE BOARD OF SUPERVISORS |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
||||||||||
|
|
ATTN: CLAIMS DIVISION |
|
|
|
|
|
|
|
|
|||||
|
|
P . O . BOX 1628, 4080 LEMON ST, 1S T FL. |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
||||||||
|
|
RIVERSIDE, CA . 92502 - 1628 |
(951) 955 - 1060 |
|
|
|
TIME STAMP HERE |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. FULL NAME OF CLAIMANT |
|
|
|
|
|
|
8. WHY DO YOU CLAIM THE COUNTY IS RESPONSIBLE? |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. MAILING ADDRESS |
(STREET/P O BOX) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
|
|
|
|
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
HOME TELEPHONE |
|
|
|
BUSINESS TELEPHONE |
|
9. NAMES OF ANY COUNTY EMPLOYEES (AND THEIR DEPARTMENTS) INVOLVED IN |
|||||||||
|
|
|
|
|
|
|
|
|
INJURY OR DAMAGE (IF APPLICABLE). |
||||||
( |
) |
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
3. WHEN DID DAMAGE OR INJURY OCCUR (PLEASE BE EXACT) |
|
|
NAME: |
|
DEPARTMENT: |
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||
4. WHERE DID DAMAGE OR INJURY OCCUR? |
|
|
|
|
NAME: |
|
DEPARTMENT: |
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
STREET |
CITY |
|
|
STATE |
|
ZIP CODE |
10. WITNESSESS TO DAMAGE OR INJURY: LIST ALL PERSONS AND ADDRESSES OF |
||||||||
|
|
|
|
|
|
|
|
|
PERSONS KNOWN TO HAVE INFORMATION: |
||||||
|
|
|
|
|
|
|
|
|
|
||||||
5. DESCRIBE IN DETAIL HOW DAMAGE OR INJURY OCCURRED: |
|
|
NAME |
|
|
|
|
PHONE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
11. LIST DAMAGES INCURRED TO DATE (attach copies of receipts or repair estimates) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
6. WERE POLICE OR PARAMEDICS CALLED? |
YES |
|
NO |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|||||||
7. IF PHYSICIAN/HOSPITAL WAS VISITED DUE TO INJURY, INCLUDE DATE OF FIRST VISIT |
|
|
|
|
|
|
|
||||||||
AND HOSPITAL’S NAME, ADDRESS AND PHONE NUMBER: |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
DATE OF FIRST VISIT |
|
|
|
PHYSICIAN’S/HOSPITAL’S NAME |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
PHYSICIAN’S/HOSPITAL’S ADDRESS |
|
PHONE: |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
TOTAL DAMAGES TO DATE |
TOTAL ESTIMATED PROSPECTIVE DAMAGES |
|||||
|
|
|
|
( |
) |
|
|
|
$_______________________ |
$_______________________________________ |
|
||||
|
|
|
|
|
|||||||||||
THIS CLAIM MUST BE SIGNED TO BE VALID. |
|
NOTE: PRESENTATION OF A FALSE CLAIM IS A FELONY (PENAL CODE SECTION 72.) |
|||||||||||||
W A R N I N G :
CLAIMS FOR DEATH, INJURY TO PERSON OR TO PERSONAL PROPERTY MUST BE FILED NOT LATER THAN SIX (6) MONTHS AFTER THE OCCURRENCE. (GOVERNMENT CODE SECTION 911.2)
ALL OTHER CLAIMS FOR DAMAGES MUST BE FILED NOT LATER THAN ONE (1) YEAR AFTER THE OCCURRENCE. (GOVERNMENT CODE SECTION 911.2)
SUBJECT TO CERTAIN EXCEPTIONS. YOU HAVE ONLY SIX (6) MONTHS FROM THE DATE OF THE WRITTEN NOTICE OF REJECTION OF YOUR CLAIM TO FILE A COURT ACTION. (GOVERNMENT CODE SECTION 945.6)
IF WRITTEN NOTICE OF REJECTION OF YOUR CLAIM IS NOT GIVEN, YOU HAVE TWO (2) YEARS FROM ACCRUAL OF THE CAUSE OF ACTION TO FILE A COURT ACTION. (GOVERNMENT CODE SECTION 945.6)
12. CLAIMANT OR PERSON FILING ON HIS/HER BEHALF
13. PRINT OR TYPE NAME |
DATE |
SIGNATURE |
RELATIONSHIP TO CLAIMANT |
REVISED: 6/26/2008