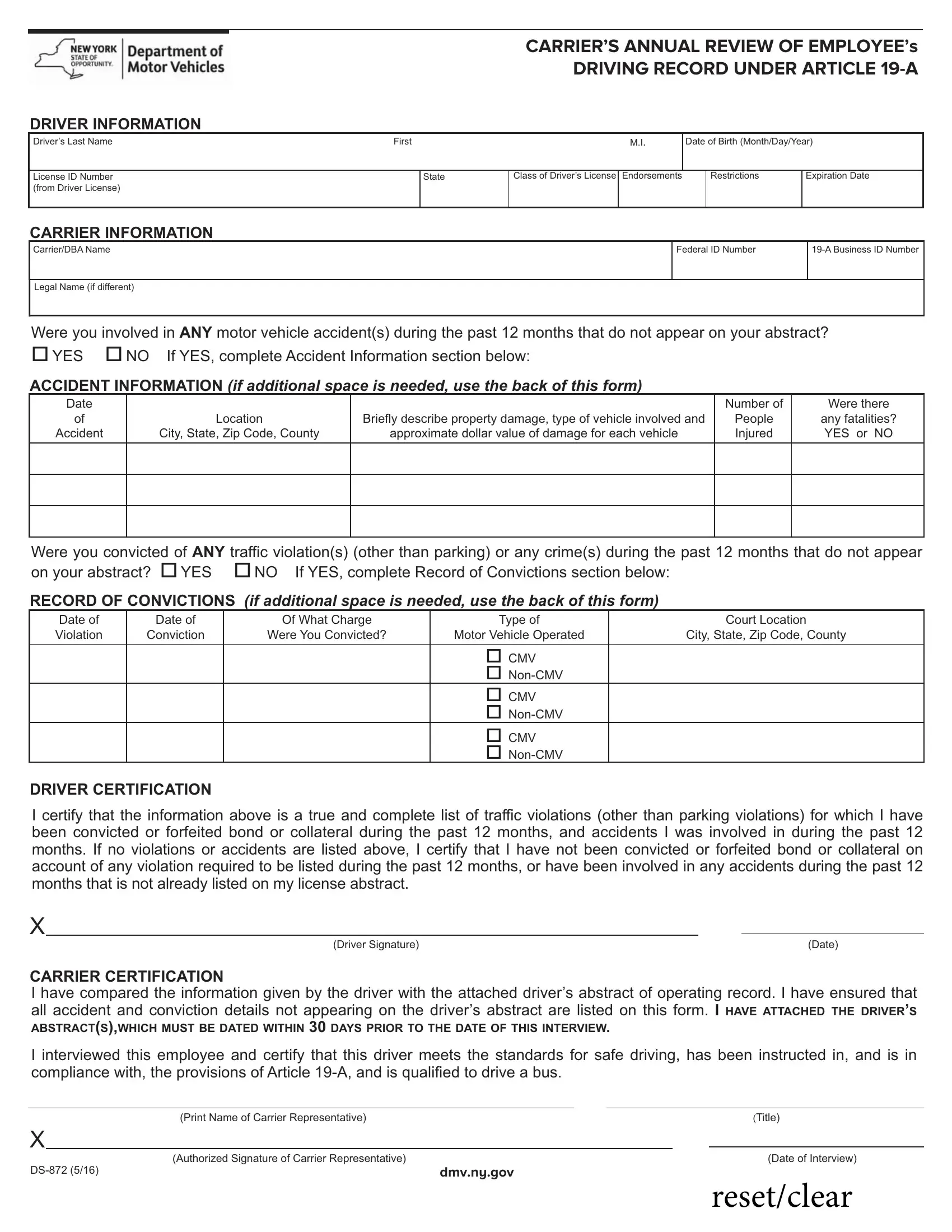

If you want to fill out nys dmv form ds 872, you don't need to download any kind of programs - just make use of our online tool. In order to make our editor better and easier to use, we consistently work on new features, with our users' feedback in mind. If you are seeking to start, here is what it will require:
Step 1: First, access the tool by pressing the "Get Form Button" above on this page.
Step 2: With our handy PDF tool, you can accomplish more than simply fill out blanks. Edit away and make your documents appear high-quality with customized textual content put in, or adjust the original content to excellence - all supported by the capability to incorporate just about any images and sign the PDF off.
Completing this form requires attentiveness. Make sure that all mandatory areas are done properly.
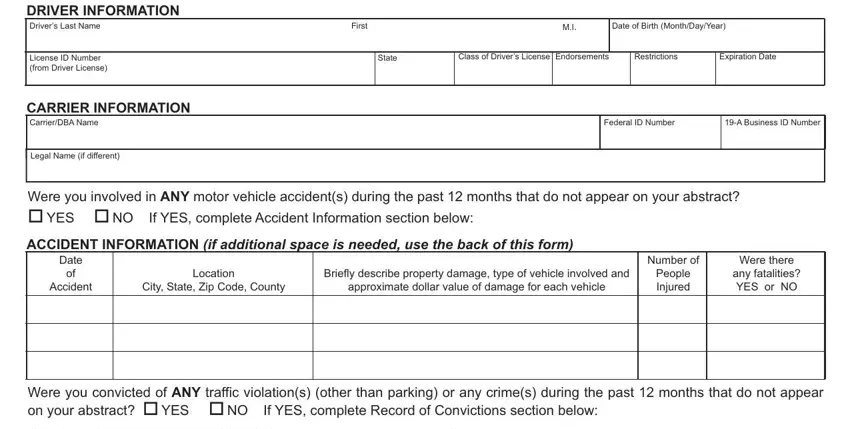
1. To start off, while filling in the nys dmv form ds 872, start out with the page that includes the following blanks:
2. Just after filling in the last step, go to the next stage and fill in the essential particulars in these blank fields - Date of Violation, Date of Conviction, Of What Charge, Were You Convicted, Type of, Court Location, Motor Vehicle Operated, City State Zip Code County, CMV NonCMV CMV NonCMV CMV, DRIVER CERTIFICATION, I certify that the information, Driver Signature, Date, and CARRIER CERTIFICATION I have.
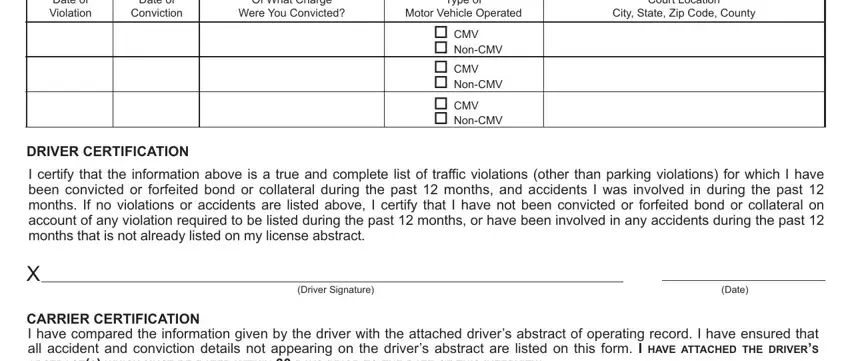
A lot of people frequently make some mistakes while completing Motor Vehicle Operated in this part. Ensure you double-check whatever you type in right here.
3. Completing I interviewed this employee and, Print Name of Carrier, Title, Authorized Signature of Carrier, dmvnygov, Date of Interview, and resetclear is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Step 3: Ensure that your details are accurate and then click on "Done" to finish the task. Create a free trial subscription at FormsPal and gain direct access to nys dmv form ds 872 - available inside your personal account. FormsPal ensures your information confidentiality with a secure method that never saves or distributes any sort of sensitive information provided. Be assured knowing your docs are kept safe each time you work with our tools!