

Handling PDF files online is definitely very easy with our PDF editor. Anyone can fill out deu rating request form here in a matter of minutes. Our tool is continually evolving to present the best user experience achievable, and that is because of our commitment to constant improvement and listening closely to comments from users. With some easy steps, you are able to start your PDF journey:
Step 1: Simply click the "Get Form Button" above on this webpage to access our form editor. Here you will find everything that is needed to work with your document.
Step 2: The tool lets you modify your PDF form in a range of ways. Change it with customized text, correct what is already in the file, and add a signature - all at your convenience!
To be able to finalize this PDF form, ensure that you enter the necessary details in each and every field:
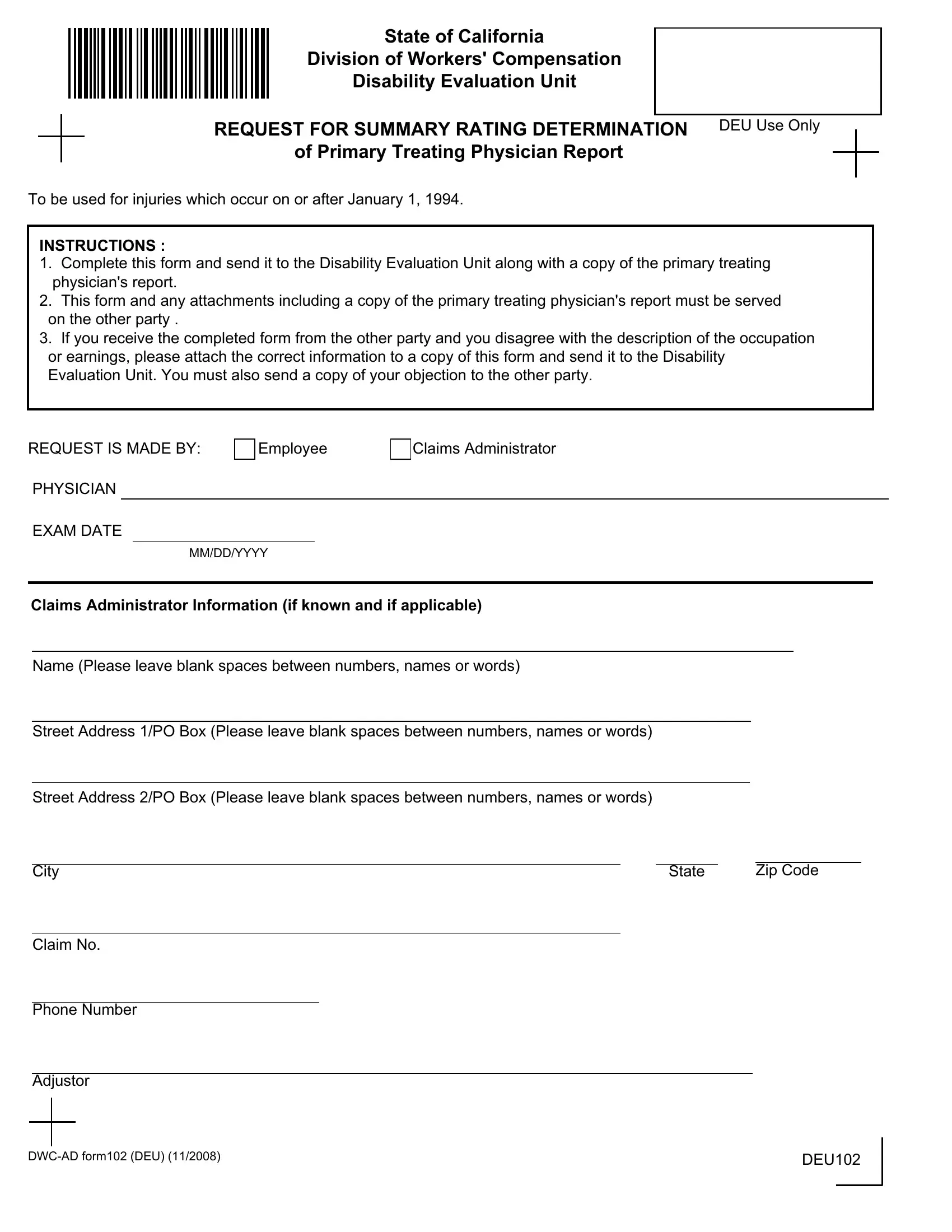
1. First, when completing the deu rating request form, start out with the area with the next blank fields:
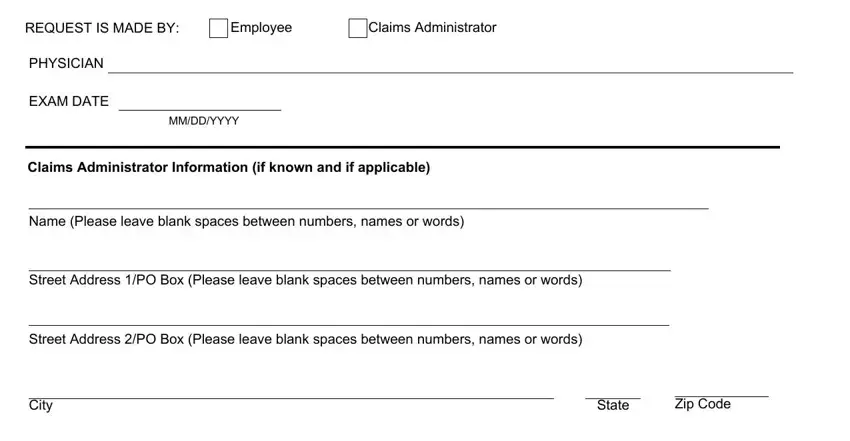
2. When the last part is complete, you're ready to insert the essential details in Claim No, Phone Number, Adjustor, DWCAD form DEU, and DEU so that you can move forward to the next step.
3. In this particular part, check out Employee, Mrs, First Name, Last Name, Street Address PO Box Please leave, Street Address PO Box Please leave, International Address Please leave, State, Zip Code, City, Date of Injury, Date of Birth, MMDDYYYY, and MMDDYYYY. All these will need to be taken care of with utmost accuracy.
4. This next section requires some additional information. Ensure you complete all the necessary fields - SSN Numbers Only, Case No, Employer, Nature of Employers Business, Job Title, DESCRIBE THE GENERAL DUTIES OF THE, WEEKLY GROSS EARNINGS are less, and Attach a wage statementDLSR if - to proceed further in your process!
Those who work with this PDF frequently make some errors when filling out WEEKLY GROSS EARNINGS are less in this section. You should definitely go over everything you enter right here.
5. The pdf needs to be completed by filling in this section. Further one can find a comprehensive list of blanks that need to be completed with correct details to allow your form usage to be complete: I served a copy of this Request, PROOF OF SERVICE BY MAIL, Name of Employee, Address, City, State, Zip Code, by placing a true copy enclosed in, and Signature.
Step 3: Prior to addressing the next step, it's a good idea to ensure that all blanks have been filled in as intended. As soon as you think it is all good, press “Done." Go for a 7-day free trial option with us and obtain immediate access to deu rating request form - download or edit inside your personal account page. At FormsPal.com, we aim to make sure your information is kept protected.