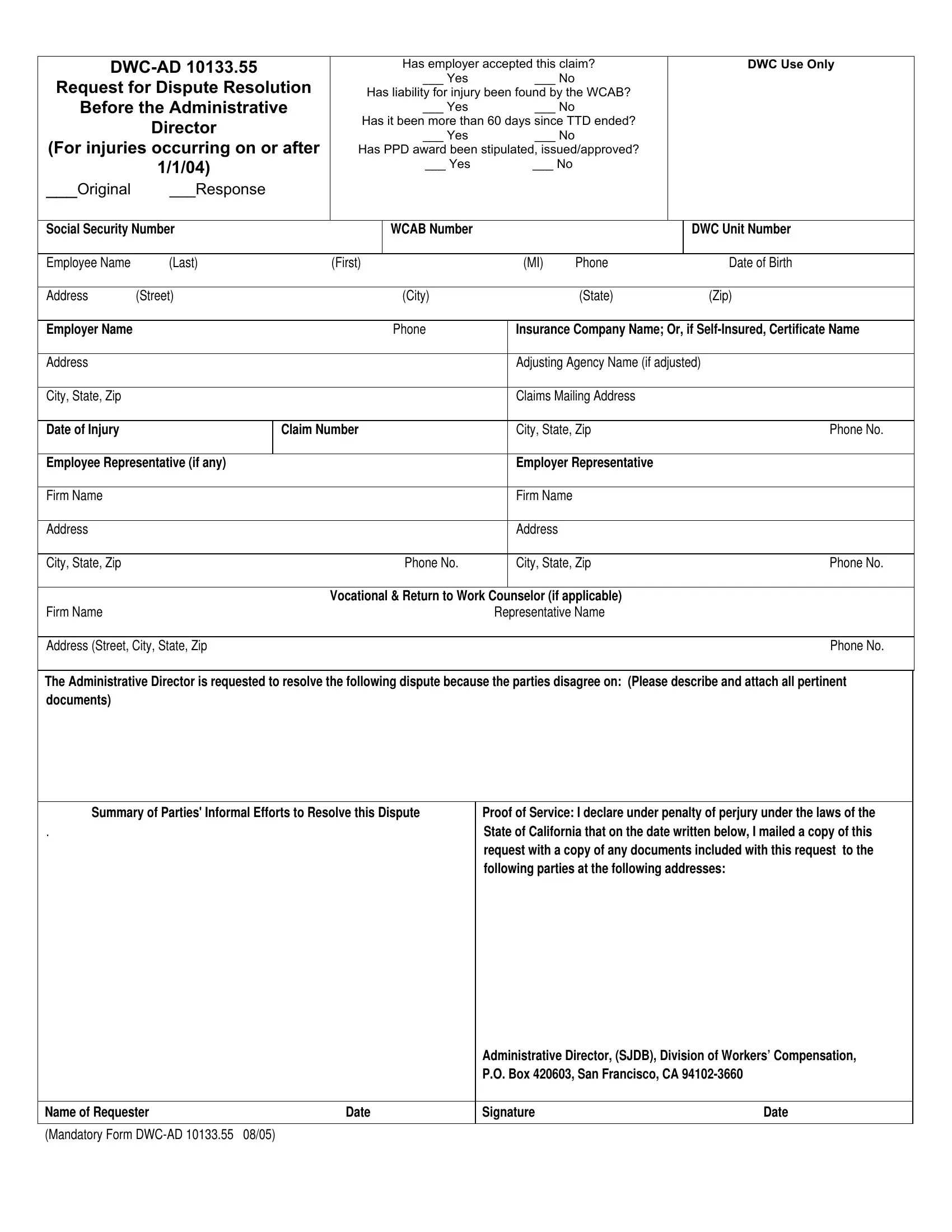
The DWC-AD 10133.55 form serves as a crucial document within the realm of workers' compensation in California, specifically designed to facilitate the dispute resolution process when disagreements arise regarding the acceptance of a claim, liability for an injury, the conclusion of temporary total disability (TTD) payments, or the issuance/approval of permanent partial disability (PPD) awards. This form, utilized exclusively by the Workers' Compensation Appeals Board (WCAB) and the Administrative Director, encompasses fields that capture essential information such as the employer's and employee's details, insurance or self-insurance certificate name, adjusting agency, and representatives of both parties, among others. It sets a procedural framework for both parties to concisely document their standpoints, summarize their informal efforts to reach a resolution, and officially request the intervention of the Administrative Director. Moreover, it stipulates the mandatory provision of proof of service to ensure that all involved parties are properly notified. The specific inclusion of checkboxes to state whether the claim has been accepted by the employer, if liability has been established, the status of TTD, and the agreement or issuance of a PPD award, alongside the provision for attaching additional pertinent documentation and detailing the nature of the dispute, underscores the exhaustive approach adopted for dispute resolution in workers' compensation cases post-injuries occurring on or after January 1, 2004.
| Question | Answer |
|---|---|
| Form Name | Form Dwc Ad 10133 55 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 10133_55Form_ Final dwc ad 1013355 instructions form |
|
Has employer accepted this claim? |
|
DWC Use Only |
||||||
Request for Dispute Resolution |
|
___ Yes |
|
___ No |
|
|
|
||
Has liability for injury been found by the WCAB? |
|
|
|||||||
Before the Administrative |
|
___ Yes |
|
___ No |
|
|
|
||
|
Director |
Has it been more than 60 days since TTD ended? |
|
|
|||||
|
|
___ Yes |
|
___ No |
|
|
|
||
(For injuries occurring on or after |
|
|
|
|
|
||||
Has PPD award been stipulated, issued/approved? |
|
|
|||||||
|
1/1/04) |
|
|
___ Yes |
|
___ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
___Original |
___Response |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Social Security Number |
|
WCAB Number |
|
|
|
|
DWC Unit Number |
||
|
|
|
|
|
|
|
|
|
|
Employee Name |
(Last) |
(First) |
|
(MI) |
Phone |
|
Date of Birth |
||
|
|
|
|
|
|
|
|
|
|
Address |
(Street) |
|
(City) |
|
|
(State) |
|
(Zip) |
|
|
|
|
|
|
|
|
|||
Employer Name |
|
|
|
Phone |
|
Insurance Company Name; Or, if |
|||
|
|
|
|
|
|
|
|||
Address |
|
|
|
|
|
Adjusting Agency Name (if adjusted) |
|||
|
|
|
|
|
|
|
|
|
|
City, State, Zip |
|
|
|
|
|
Claims Mailing Address |
|
|
|
|
|
|
|
|
|
|
|||
Date of Injury |
|
Claim Number |
|
City, State, Zip |
|
Phone No. |
|||
|
|
|
|
|
|
|
|
||
Employee Representative (if any) |
|
|
|
Employer Representative |
|
|
|||
|
|
|
|
|
|
|
|
|
|
Firm Name |
|
|
|
|
|
Firm Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
City, State, Zip |
|
|
|
Phone No. |
|
City, State, Zip |
|
Phone No. |
|
|
|
|
|
|
|
|
|||
|
|
|
Vocational & Return to Work Counselor (if applicable) |
|
|
||||
Firm Name |
|
|
|
|
Representative Name |
|
|
||
|
|
|
|
|
|
|
|
||
Address (Street, City, State, Zip |
|
|
|
|
|
|
Phone No. |
||
|
|
|
|
|
|
|
|
|
|
The Administrative Director is requested to resolve the following dispute because the parties disagree on: (Please describe and attach all pertinent documents)
Summary of Parties' Informal Efforts to Resolve this Dispute |
Proof of Service: I declare under penalty of perjury under the laws of the |
||
. |
|
State of California that on the date written below, I mailed a copy of this |
|
|
|
request with a copy of any documents included with this request to the |
|
|
|
following parties at the following addresses: |
|
|
|
Administrative Director, (SJDB), Division of Workers’ Compensation, |
|
|
|
P.O. Box 420603, San Francisco, CA |
|
|
|
|
|
Name of Requester |
Date |
Signature |
Date |
|
|
|
|
(Mandatory Form