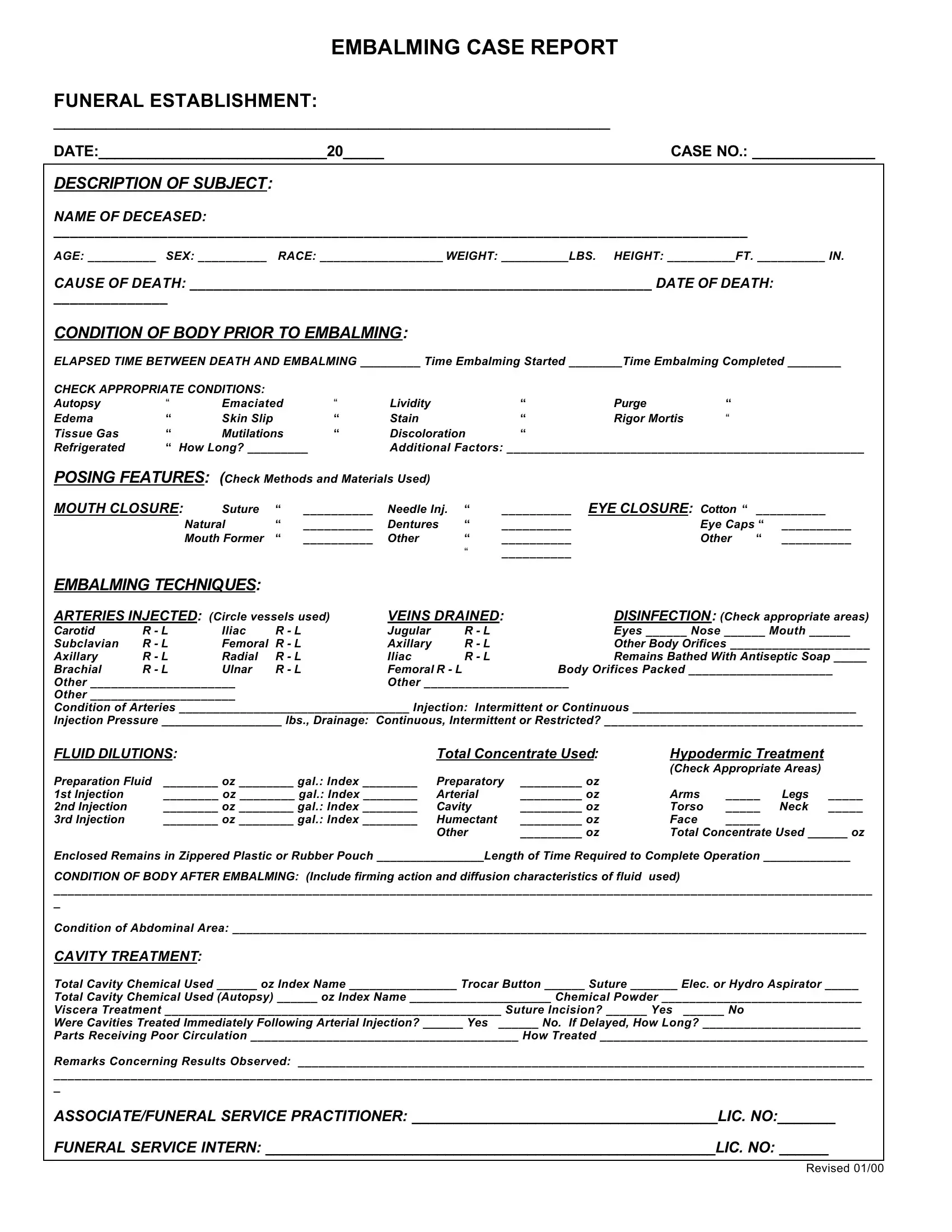
In the meticulous domain of funeral services, the Embalming Case Report form constitutes an essential document, outlining comprehensive details necessary for embalming procedures. From identifying information about the deceased, including name, age, sex, race, weight, and height, to specifics of cause and date of death, this form captures critical data. It further delves into the condition of the body prior to embalming, noting any signs of autopsy, edema, rigor mortis, or other pertinent conditions that may affect the embalming process. The techniques employed, arteries injected, veins drained, and the fluids used are meticulously documented, ensuring a precise account of the embalming approach. Additionally, this report encompasses cavity treatment details, the condition of the body post-embalming, and the use of protective clothing by the professionals involved. It also provides space for noting any personal property received with the body and its final disposition, underscoring the form's role in both the practical and respectful treatment of the deceased. Illustrated through its thoroughness, the Embalming Case Report form serves as a critical tool in maintaining the highest standards of care in funeral services.
| Question | Answer |
|---|---|
| Form Name | Embalming Case Report Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | blank embalming case report, printable embalming case report forms, embalming case report pdf, embalming case report |
EMBALMING CASE REPORT
FUNERAL ESTABLISHMENT:
_____________________________________________________
DATE:____________________________20_____ |
CASE NO.: _______________ |
|
|
DESCRIPTION OF SUBJECT: |
|
NAME OF DECEASED:
_____________________________________________________________________________________
AGE: __________ SEX: __________ RACE: __________________ WEIGHT: __________LBS. HEIGHT: __________FT. __________ IN.
CAUSE OF DEATH: _________________________________________________________ DATE OF DEATH:
______________
CONDITION OF BODY PRIOR TO EMBALMING:
ELAPSED TIME BETWEEN DEATH AND EMBALMING _________ Time Embalming Started ________Time Embalming Completed ________
CHECK APPROPRIATE CONDITIONS: |
|
|
|
|
|
|
|
|
|
||
Autopsy |
“ |
Emaciated |
“ |
Lividity |
|
“ |
Purge |
“ |
|
|
|
Edema |
“ |
Skin Slip |
|
“ |
Stain |
|
“ |
Rigor Mortis |
“ |
|
|
Tissue Gas |
“ |
Mutilations |
“ |
Discoloration |
“ |
|
|
|
|
||
Refrigerated |
“ How Long? _________ |
Additional Factors: ____________________________________________________ |
|||||||||
POSING FEATURES: (Check Methods and Materials Used) |
|
|
|
|
|
|
|||||
MOUTH CLOSURE: |
Suture |
“ |
__________ |
Needle Inj. |
“ |
__________ |
EYE CLOSURE: |
Cotton “ |
__________ |
||
|
|
Natural |
“ |
__________ |
Dentures |
“ |
__________ |
|
Eye Caps “ |
__________ |
|
|
|
Mouth Former |
“ |
__________ |
Other |
“ |
__________ |
|
Other |
“ |
__________ |
|
|
|
|
|
|
“ |
__________ |
|
|
|
|
EMBALMING TECHNIQUES: |
|
|
|
|
|
|
|
|
|
||
ARTERIES INJECTED: (Circle vessels used) |
VEINS DRAINED: |
DISINFECTION: (Check appropriate areas) |
|||||||||
Carotid |
R - L |
Iliac |
R - L |
|
Jugular |
R - L |
|
Eyes ______ Nose ______ Mouth ______ |
|||
Subclavian |
R - L |
Femoral |
R - L |
|
Axillary |
R - L |
|
Other Body Orifices ____________________ |
|||
Axillary |
R - L |
Radial |
R - L |
|
Iliac |
R - L |
|
Remains Bathed With Antiseptic Soap _____ |
|||
Brachial |
R - L |
Ulnar |
R - L |
|
Femoral R - L |
|
Body Orifices Packed _____________________ |
||||
Other _____________________ |
|
|
Other _____________________ |
|
|
|
|
||||
Other _____________________ |
|
|
|
|
|
|
|
|
|
||
Condition of Arteries __________________________________ Injection: Intermittent or Continuous _________________________________
Injection Pressure __________________ lbs., Drainage: Continuous, Intermittent or Restricted? _____________________________________
FLUID DILUTIONS: |
Total Concentrate Used: |
Hypodermic Treatment |
|
||||
|
|
|
|
(Check Appropriate Areas) |
|
||
Preparation Fluid |
________ oz ________ gal.: Index ________ |
Preparatory |
_________ oz |
|
|
|
|
1st Injection |
________ oz ________ gal.: Index ________ |
Arterial |
_________ oz |
Arms |
_____ |
Legs |
_____ |
2nd Injection |
________ oz ________ gal.: Index ________ |
Cavity |
_________ oz |
Torso |
_____ |
Neck |
_____ |
3rd Injection |
________ oz ________ gal.: Index ________ |
Humectant |
_________ oz |
Face |
_____ |
|
|
|
|
Other |
_________ oz |
Total Concentrate Used ______ oz |
|||
Enclosed Remains in Zippered Plastic or Rubber Pouch ________________Length of Time Required to Complete Operation _____________
CONDITION OF BODY AFTER EMBALMING: (Include firming action and diffusion characteristics of fluid used)
_____________________________________________________________________________________________________________________
_
Condition of Abdominal Area: ____________________________________________________________________________________________
CAVITY TREATMENT:
Total Cavity Chemical Used ______ oz Index Name ________________ Trocar Button ______ Suture _______ Elec. or Hydro Aspirator _____
Total Cavity Chemical Used (Autopsy) ______ oz Index Name _____________________ Chemical Powder _____________________________
Viscera Treatment _________________________________________________ Suture Incision? ______ Yes ______ No
Were Cavities Treated Immediately Following Arterial Injection? ______ Yes ______ No. If Delayed, How Long? _______________________
Parts Receiving Poor Circulation _______________________________________ How Treated _______________________________________
Remarks Concerning Results Observed: __________________________________________________________________________________
_____________________________________________________________________________________________________________________
_
ASSOCIATE/FUNERAL SERVICE PRACTITIONER: _____________________________________LIC. NO:_______
FUNERAL SERVICE INTERN: _______________________________________________________LIC. NO: ______
REVISED 01/00
PROTECTIVE CLOTHING/EQUIPMENT USED:
Gloves |
“ |
Face Mask |
“ |
Boots |
“ |
Goggles |
“ |
Face Shield |
“ |
Head Cover |
“ |
Gown |
“ |
Medigard Glove |
“ |
Other |
“ ____________________ |
Describe Other Items Used: ___________________________________________________________________________________________________
___________________________________________________________________________________________________________________________
_
Was Embalming Completed Without Incident? _____Yes _____ No
If No, Give Detail to Complete Operation ___________________________________________________ Ending Time ___________________a.m./p.m.
PROPERTY RECORD:
Personal Property Received With Body (List all Items):
Clothing
___________________________________________________________________________________________________________________________
_
Jewelry _________________________________________________________________________________Cash
_______________________________
Dentures ___________________Papers
__________________________________________________________________________________________
Other Items
__________________________________________________________________________________________________________________
FINAL DISPOSITION OF PERSONAL PROPERTY:
Property Received by ______________________________________Relationship to Deceased _________________________Date ________________
ADDITIONAL REMARKS OR COMMENTS CONCERNING CASE:
_________________________________________________________________________________________________________
____
_________________________________________________________________________________________________________
____
_________________________________________________________________________________________________________
____
DISPOSITION OF HUMAN REMAINS:
Cemetery |
“ |
Mausoleum |
“ |
|
Crematory |
“ |
“ |
Receiving Funeral Home _______________________________ City & State ___________________________ |
CASKET DESCRIPTION ______________________________________OUTSIDE CONTAINER ______________________________________________
IDENTIFICATION ANATOMICAL CHART
INDICATE IDENTIFIABLE UNUSUAL MARKINGS OR CONDITIONS ON FIGURES
(Tattoo, scar, wound, fractured bone, sore, other)
1. _________________________________________ 3. ____________________________________________
2. _________________________________________ 4. ____________________________________________