
You can work with ga dol 1a easily with the help of our PDFinity® PDF editor. In order to make our tool better and easier to work with, we continuously implement new features, considering feedback coming from our users. Starting is easy! All you should do is follow the next basic steps down below:
Step 1: First of all, open the pdf tool by pressing the "Get Form Button" at the top of this site.
Step 2: The tool will allow you to modify PDF documents in a variety of ways. Modify it with personalized text, correct what is already in the document, and include a signature - all within several clicks!
As for the fields of this precise PDF, here is what you should do:
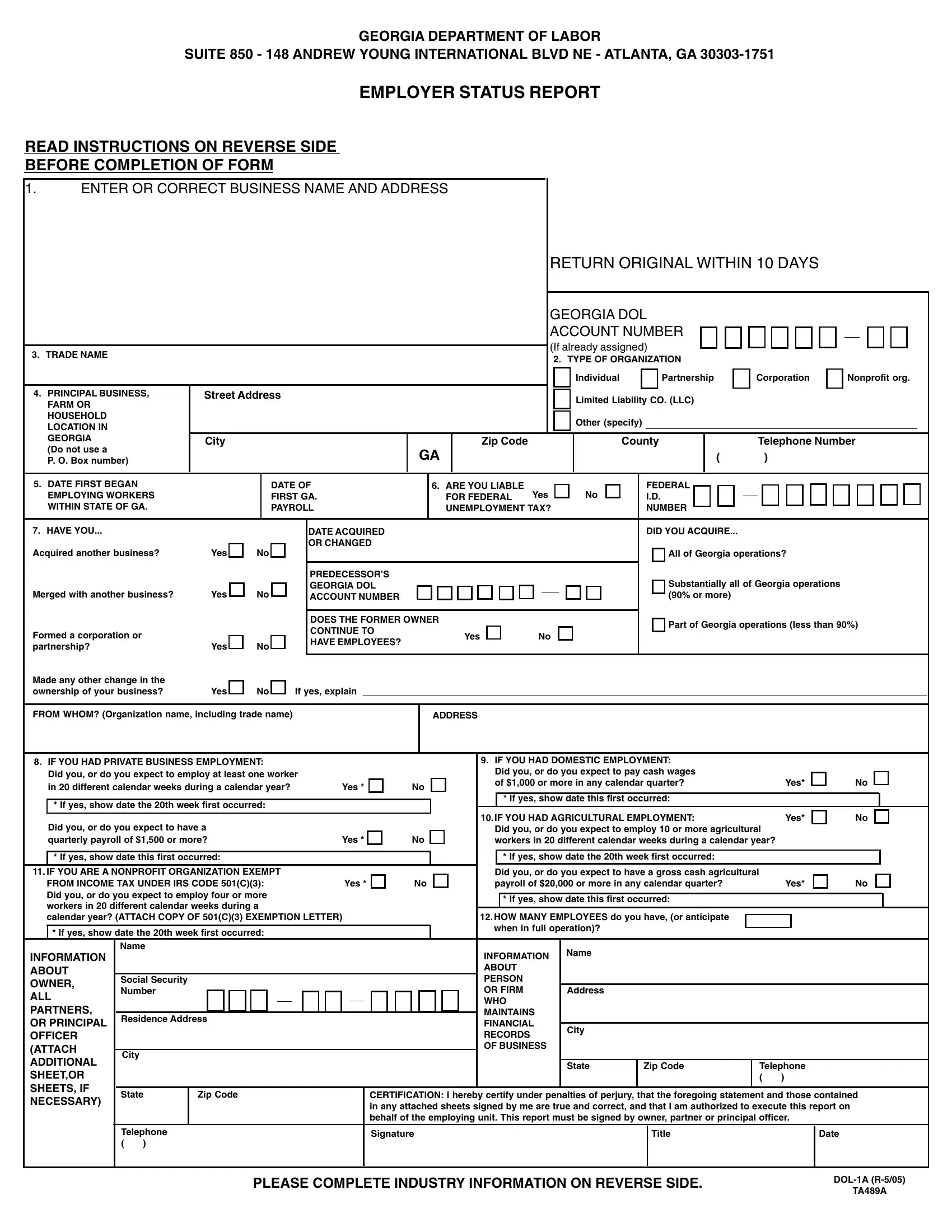
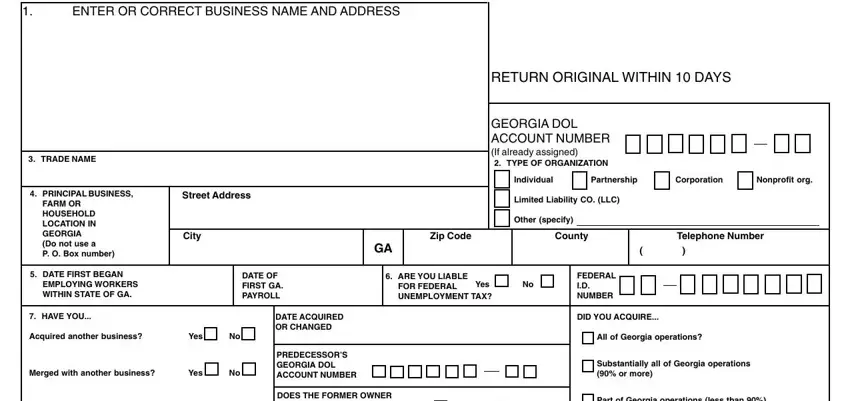
1. You will need to complete the ga dol 1a accurately, hence be mindful when working with the parts including all these blank fields:
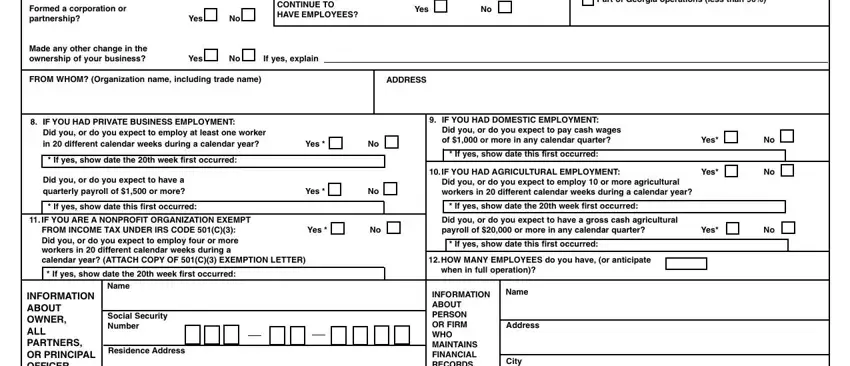
2. When the last section is completed, you're ready to insert the required particulars in Part of Georgia operations less, Formed a corporation or partnership, Yes, DOES THE FORMER OWNER CONTINUE TO, Yes No, Made any other change in the, Yes, If yes explain, FROM WHOM Organization name, ADDRESS, IF YOU HAD PRIVATE BUSINESS, If yes show date the th week, Did you or do you expect to have a, If yes show date this first, and Yes in order to proceed further.
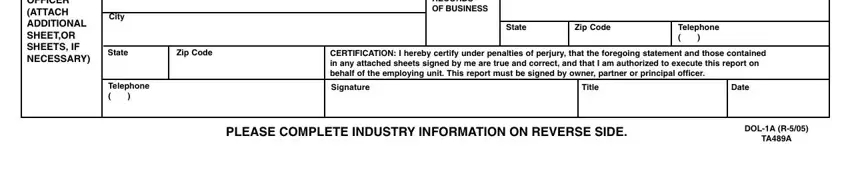
3. Through this stage, look at INFORMATION ABOUT OWNER ALL, City, State, Zip Code, Telephone, INFORMATION ABOUT PERSON OR FIRM, City, State, Zip Code, Telephone, CERTIFICATION I hereby certify, Signature, Title, Date, and PLEASE COMPLETE INDUSTRY. These are required to be taken care of with utmost precision.
4. All set to fill in the next portion! Here you have these Provide the following information, B Check the box that best, business activities, Agriculture Forestry Fishing, Manufacturing Transportation, Principal Services Rendered, Principal Products Mfg, Grown, Sold, If Transportation Trucking, D If this report includes, Central Administration Research, Storage warehouse Other specify, FOR ASSISTANCE call the Industry, and IMPORTANT This report must be form blanks to fill out.
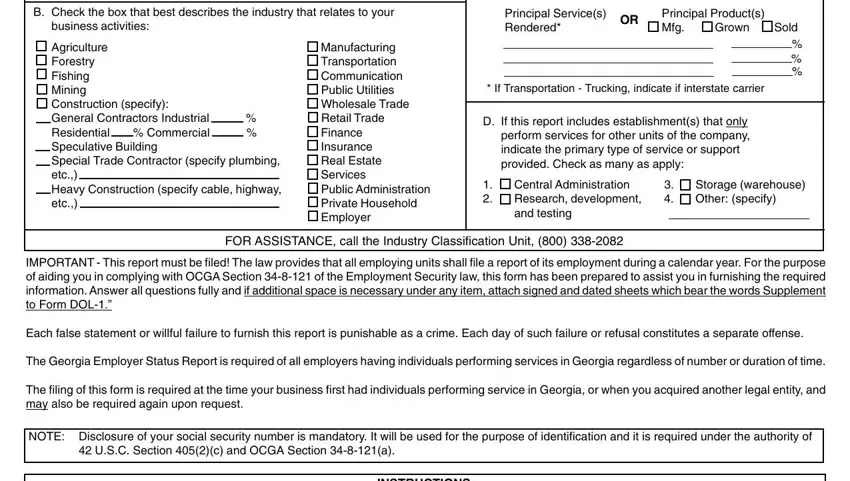
Always be very attentive while filling in Sold and Storage warehouse Other specify, because this is the part in which many people make a few mistakes.
Step 3: Just after going through your completed blanks, press "Done" and you are all set! Get hold of the ga dol 1a once you register at FormsPal for a 7-day free trial. Conveniently access the pdf form inside your personal account page, together with any edits and changes conveniently kept! When you use FormsPal, you'll be able to fill out documents without worrying about data leaks or data entries being distributed. Our secure software makes sure that your private information is stored safe.