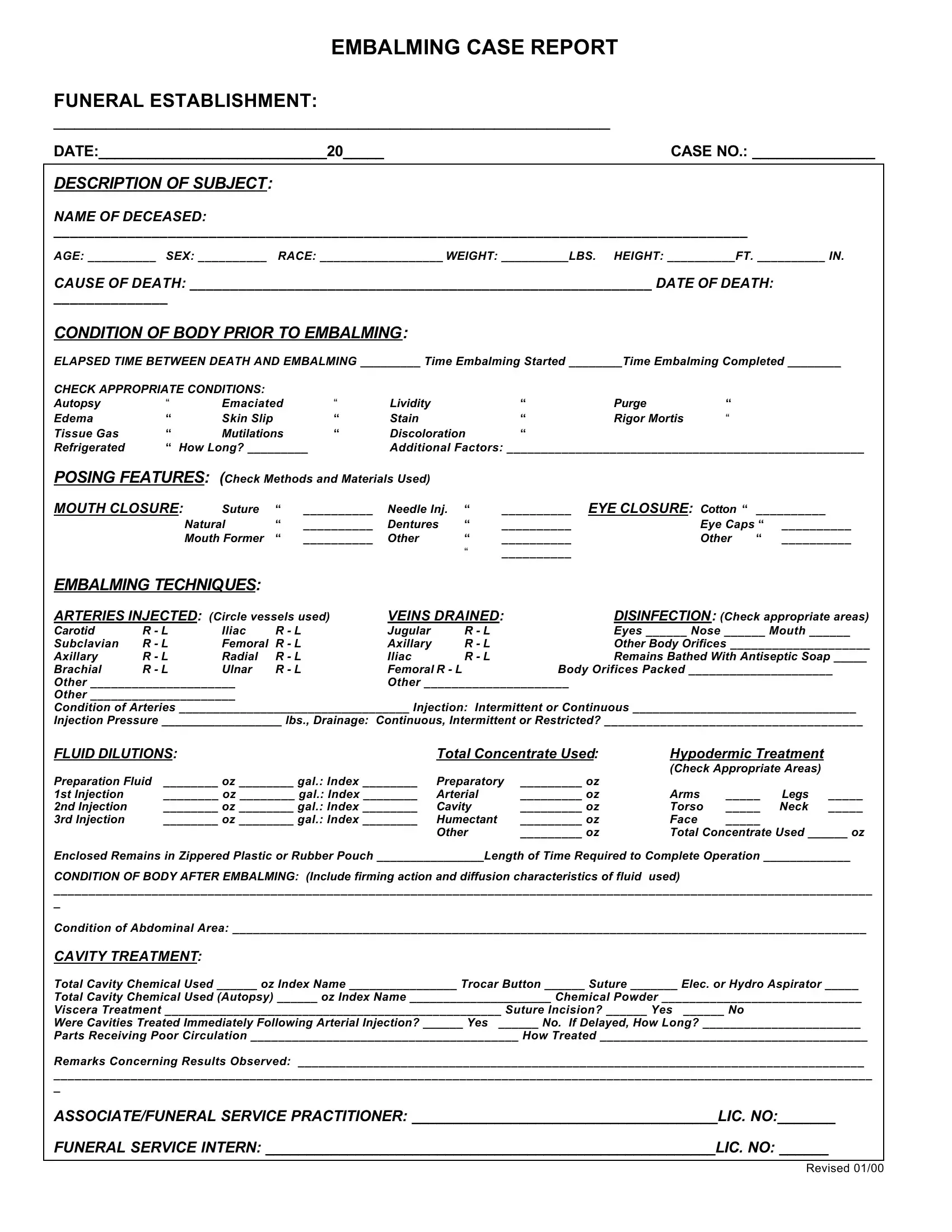
In the meticulous domain of funeral services, the Embalming Case Report form constitutes an essential document, outlining comprehensive details necessary for embalming procedures. From identifying information about the deceased, including name, age, sex, race, weight, and height, to specifics of cause and date of death, this form captures critical data. It further delves into the condition of the body prior to embalming, noting any signs of autopsy, edema, rigor mortis, or other pertinent conditions that may affect the embalming process. The techniques employed, arteries injected, veins drained, and the fluids used are meticulously documented, ensuring a precise account of the embalming approach. Additionally, this report encompasses cavity treatment details, the condition of the body post-embalming, and the use of protective clothing by the professionals involved. It also provides space for noting any personal property received with the body and its final disposition, underscoring the form's role in both the practical and respectful treatment of the deceased. Illustrated through its thoroughness, the Embalming Case Report form serves as a critical tool in maintaining the highest standards of care in funeral services.
| Question | Answer |
|---|---|
| Form Name | Embalming Case Report Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | blank embalming case report, printable embalming case report forms, embalming case report pdf, embalming case report |
