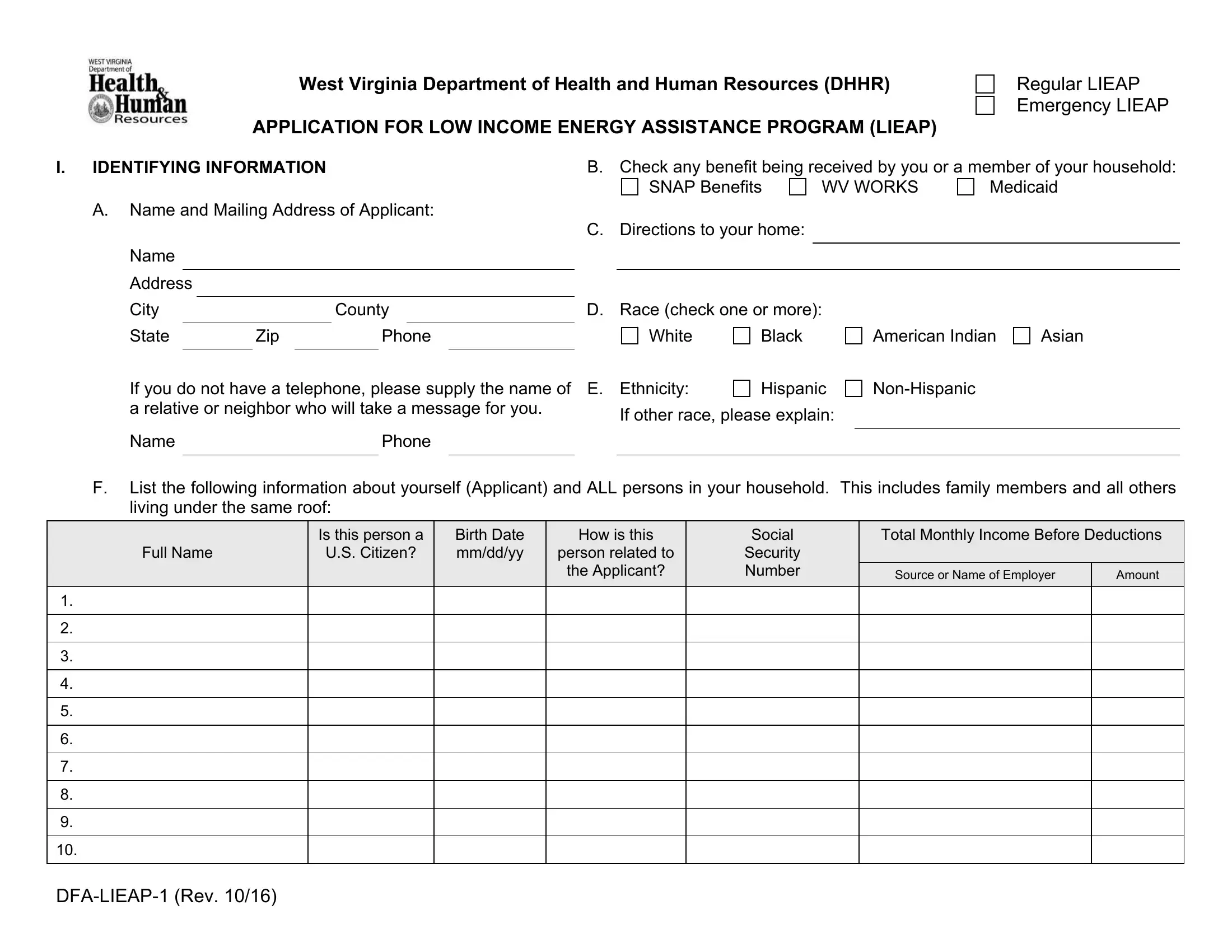
In an effort to support those facing financial difficulties in managing home heating costs, the West Virginia Department of Health and Human Resources (DHHR) provides the Low Income Energy Assistance Program (LIEAP). This critical initiative comprises both Regular LIEAP and Emergency LIEAP segments, designed to offer financial assistance to eligible low-income households struggling to keep their homes warm during the harsh winter months. Applicants are required to provide comprehensive personal and household information, including details on income, household composition, and heating sources, to ensure accurate and fair assistance distribution. Additionally, the form inquires about current living arrangements, disabilities within the household, and specifics regarding the main heating and electricity sources to tailor support effectively. The application emphasizes the importance of honesty and compliance, highlighting potential repercussions for false statements and underscoring the cooperative relationship between the DHHR, utility companies, and applicants. The process is meticulously structured to ensure that those who are most in need receive timely aid to mitigate the risks associated with cold weather, thereby reinforcing the program's commitment to community welfare and support.
| Question | Answer |
|---|---|
| Form Name | Emergency Lieap Wv Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | wv lieap application, wv application lieap online, wv emergency lieap, wv lieap application 2021 |
