When new patients first encounter the comprehensive and meticulously detailed New Patient Information form provided by Emory Healthcare, they embark on a vital step towards receiving personalized and efficient care. This form is ingeniously designed to gather a wide spectrum of personal and medical information, ensuring that all bases are covered -- from basic contact information and referral details to a precise history of the patient’s present complaints, social history, and past medical or surgical history. Patients are requested to provide a thorough account of their condition, including symptom descriptions, pain levels with a unique orthopedic pain chart, and the treatments they have undergone, which further aids in crafting a targeted care plan. Moreover, it encompasses inquiries about the patient’s social history, lifestyle factors such as smoking and alcohol consumption, and legal questions regarding lawsuits, which could all be relevant to the patient’s health journey. The form also meticulously collects data on past medical and surgical history, current medications, and allergies, ensuring that healthcare providers have a well-rounded view of the patient’s health. This thorough approach not only streamlines the process of integrating new patients into the Emory Healthcare system but also underscores the institution’s commitment to delivering personalized and comprehensive healthcare services.
| Question | Answer |
|---|---|
| Form Name | Emory Healthcare New Patient Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | emory patient form, emory new patient forms, emory neurology new patient forms, emory healthcare new patient |
NEW PATIENT INFORMATION FORM
Please print all information. All blanks must be filled to allow us to serve you quickly and efficiently.
Thank you for your cooperation.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date: |
|
|
|
|
|
|
|
|
Date of Birth: |
|
|
|
|
|
|
|
|||||
|
|
Patient Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Phone: Home: ( |
) |
|
|
|
|
Work: ( |
) |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
How were you referred to The Emory Spine Center: Physician |
Patient / Friend |
Health Connection |
|
|
|||||||||||||||||
|
|
Workers Comp |
Emory Reputation Insurance |
Radio / TV Advertisement |
Other: |
|
|
||||||||||||||||
|
|
Referring Physician or Referral Source: |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Phone: ( |
) |
|
|
|
|
|
|
Fax: ( |
) |
|
|
|
|
|
|
|
|
||||
|
|
Do you want your medical records sent to this physician? |
Yes |
No |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Doctor:
Address:
City:
Phone: ( |
) |
|
|
Fax: ( |
) |
|
Do you want your medical records sent to this physician? |
Yes |
No |
||||
Are there any other physicians to whom you would like your medical records sent? (Please include name and address)
(Continued on next page)
SpineIntake.doc 3/20/04
Page 2
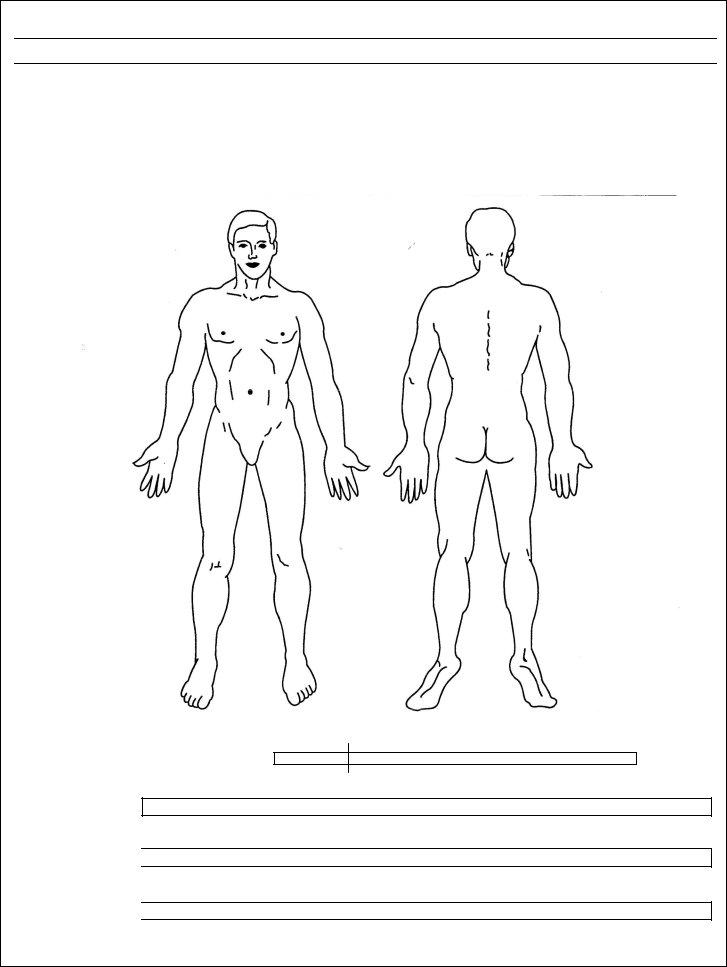
ORTHO PAIN CHART
Mark the areas on your body where you feel the described sensations using the appropriate symbol from the list below. Please include all affected areas.
|
= = = |
|
o o o |
Burning |
x x x |
|
/ / / / |
Numbness = |
= = = |
Pin & Needles = |
o o o |
Aching = |
x x x |
Stabbing = |
/ / / / |
|
= = = |
|
o o o |
|
x x x |
|
/ / / / |
RL LR
RL LR
Please indicate your current pain level by placing a line below with “0” = no pain and “10” = worst pain imaginable.
Example: Pain
0
Pain at its Worst
0
Pain at its Best |
|
|
|
(lying down, resting) |
|
0 |
|
|
|
||
Pain on Average |
|
|
|
|
|
|
|
|
|
||
|
|
0 |
|
10
10
10
10
SpineIntake.doc 3/20/04
Page 3
HISTORY OF PRESENT COMPLAINT
1. |
Age: |
|
|
2. Male |
|
Female |
3. Right Handed |
Left Handed |
|||||||||
4. |
Where is your problem located? |
Left side Right side |
|
|
|
|
|
|
|
|
|||||||
|
|
Neck |
Upper Back |
Arm/Elbow |
Shoulder |
Wrist/Hand |
|
|
|
|
|
||||||
|
|
Lower Back |
Hip |
Leg |
Knee |
Ankle |
Foot |
|
|
|
|
|
|
||||
5. |
How long have you had this problem? |
|
|
|
Since? |
|
/ |
|
/ |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
month |
|
|
day |
|
year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. Briefly, please give the details of how this problem originally started:
7.Was this from a
- Is it under workers compensation No Yes No Yes, how much?
8.Please describe your present pain now (what you feel, where, when, etc.):
9.Of the following list of treatments, please indicate the effect of those which have been used in an attempt to help
your present problem: (Check one of each)
|
|
|
|
Which type |
|
Helpful |
No Help |
Not Used |
Antiinflammatory |
|
|
|
|
|
|||
Muscle Relaxants |
|
|
|
|
|
|||
Narcotic Pain Medications |
|
|
|
|
|
|||
Hot Packs |
|
|
|
|
||||
Ice |
|
|
|
|
|
|||
Ultrasound |
|
|
|
|
|
|||
Physical Therapy Treatment |
|
|
|
|
|
|||
Cortisone Injection |
|
|
|
|
||||
Trigger Point Injection |
|
|
|
|
|
|||
Brace/Splint |
|
|
|
|
|
|||
Chiropractor |
|
|
|
|
|
|||
Acupuncture |
|
|
|
|
||||
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
(Continued on next page) |
|
|
|
|
SpineIntake.doc 3/20/04
Page 4
PAST HISTORY
10. |
Please indicate whether you have had any of the following studies for this problem: |
|
|
|||||||||||||||||
|
|
|
YES |
NO |
WHEN/WHERE |
|
|
|
YES NO |
|
|
WHEN/WHERE |
|
|
||||||
|
Regular |
|
|
|
|
|
CT Scan |
|
|
|
|
|
|
|
|
|
|
|||
|
EMG |
|
|
|
|
|
MRI |
|
|
|
|
|
|
|
|
|
|
|||
11. |
Have you had surgery for this problem in the past: (Check one) Yes No |
|
How many times? |
|
|
|||||||||||||||
|
What was the date(s) of the most recent surgery? |
|
|
, |
|
|
, |
|
|
|
|
|
|
|
|
|||||
|
Did you improve from the surgery procedure(s)? |
Yes |
No |
|
|
|
|
|
|
|
||||||||||
12. |
Have you had any past episodes of similar pain or injury? |
Yes |
No |
(please describe) |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL HISTORY
13. |
Current work status: Working full duty |
Working restricted duty (Since |
) |
Retired |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
Disabled |
( Since |
|
|
|
) Student |
Homemaker |
Unemployed |
|
|
|
|
||||||||||||||||
|
Company: |
|
|
|
|
|
|
|
Occupation: |
|
|
|
|
|
|
|
Title: |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
How long have you worked for this company? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
14. |
Marital status |
Single |
Married |
Divorced |
|
|
Widowed |
|
|
|
|
|
|
|||||||||||||||
15. |
Number of Children: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
16. |
I live: |
Alone |
|
With: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
17. |
I live in a: |
House |
|
Apartment |
Assisted living |
Nursing home |
|
|
|
|
|
|
||||||||||||||||
18. |
Are you a cigarette smoker? |
|
Yes, now Never Quit - |
How long ago did you quit? |
||||||||||||||||||||||||
|
If you answered “yes” or “quit”, how much do or did you smoke per day? |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
Less than ½ pack |
½ pack |
¾ pack |
1 pack |
|
More (How many?) |
||||||||||||||||||||||
|
How old were you when you started smoking? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
None |
|
|
|
|
|
|
|
|
|
|
||||||||||||
19. |
Do you drink any alcoholic beverages? |
(Check one) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
0 to 3 drinks per month |
|
1 to 2 drinks per day |
|
|
3 to 5 drinks per day |
|
|
|
|
|
|
||||||||||||||||
|
More than 5 drinks per day. |
How many? |
|
/ |
Alcoholic in past? |
Yes |
|
No |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
20. |
Have you ever had a problem with drug dependence? |
Yes |
|
No |
|
|
|
|
|
|
||||||||||||||||||
21. |
Are there any law suits pending or contemplated related to your problem? |
Yes |
No |
|
|
|
|
|||||||||||||||||||||
If yes, please give your attorney’s name and phone number:
SpineIntake.doc 3/20/04
|
|
|
|
|
|
|
|
|
Page 5 |
|
|
|
|
|
|
|
|
|
|||
|
MEDICAL/SURGICAL HISTORY |
|
|
|
|
|||||
|
Please choose all current and past medical conditions |
|
|
|
|
|||||
No medical problem |
Diabetes |
|
|
|
Bleeding disorders |
|||||
High blood pressure |
Thyroid disease |
|
|
|
Anemia |
|||||
Heart attack |
Stomach ulcers / Gastric Reflux |
Blood clots in legs/lung |
||||||||
Heart failure |
Irritable bowel |
|
|
|
Endometriosis |
|||||
Abnormal heart rhythm |
Stroke |
|
|
|
Ovarian cysts |
|||||
Lung disease |
Seizures |
|
|
|
Anxiety |
|||||
Tuberculosis |
Cancer – where? |
|
|
|
|
Depression |
||||
Asthma |
Kidney Failure |
|
|
|
Schizophrenia |
|||||
Bronchitis |
Kidney Stones |
|
|
|
Anorexia/bulemia |
|||||
Emphysema |
Osteoporosis |
|
|
|
Alcoholism |
|||||
Liver disease |
Osteoarthritis |
|
|
|
Seen a psychiatrist |
|||||
Hepatitis |
Rheumatoid arthritis |
|
|
|
HIV |
|||||
Are you under a doctor’s care for any other medical condition? |
Yes |
No |
|
If yes, please explain |
||||||
|
|
|
|
|
|
|||||
|
Please choose all surgeries you have had |
|
|
|
|
|||||
|
Appendix / Intestine |
|
|
|
Eyes |
|||||
|
Hernia / Colon / Rectum |
|
|
Ears |
||||||
Brain |
Hysterectomy / |
Nose |
||||||||
Heart / Pacemaker / IV Filter |
Kidneys / Bladder / Urinary |
|
|
Throat / Tonsils |
||||||
Angioplasty / Stent |
Prostate |
|
|
|
Other |
|
|
|||
Lung |
Shoulders / Arms / Hands |
> Describe |
||||||||
|
|
|
|
|
||||||
Gallbladder / Stomach |
Hips / Knees / Legs / Feet > Describe |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
List All Allergies
Substance |
|
Reaction |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
List All Current Medications
Name |
|
Dose |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Continued on next page)
SpineIntake.doc 3/20/04