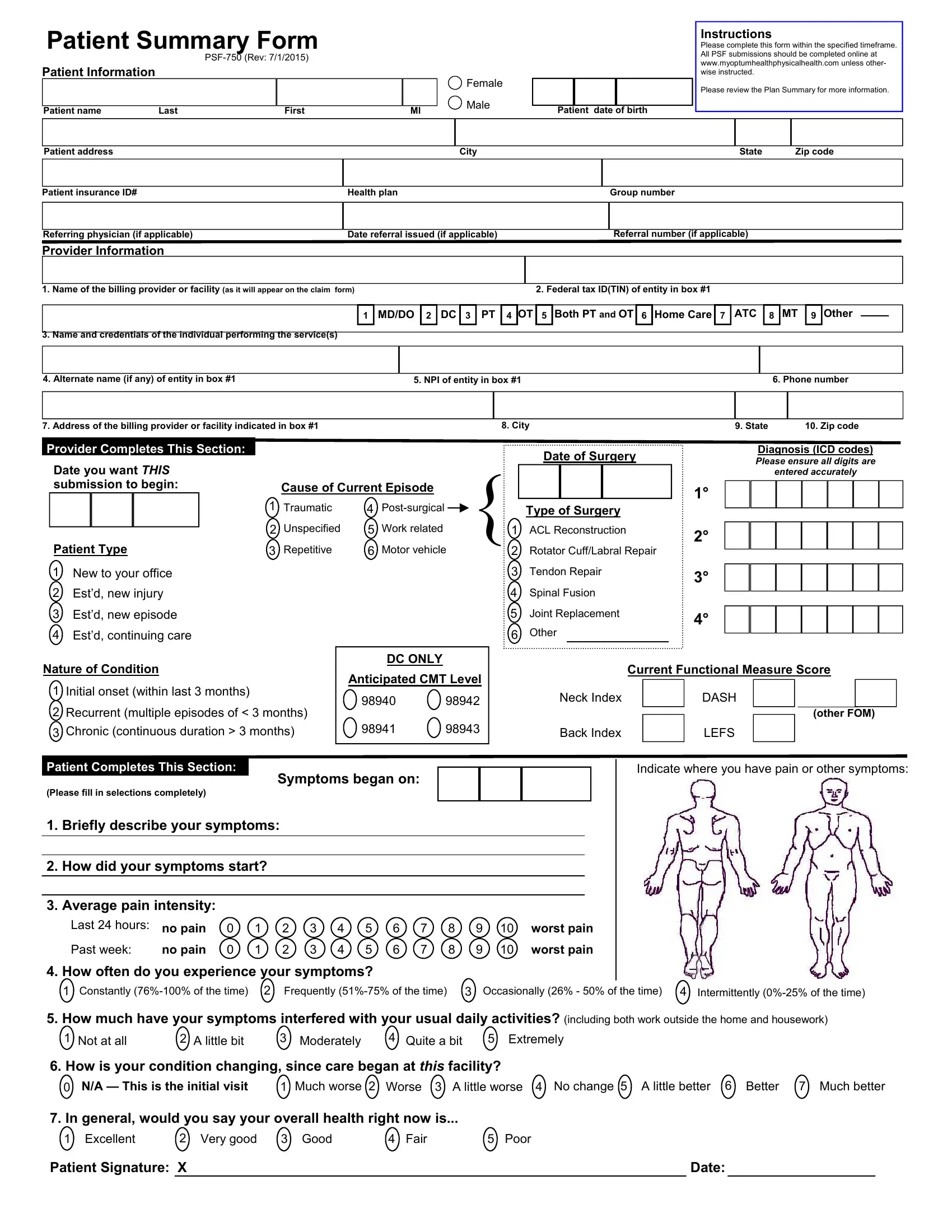
In the realm of healthcare, the transparency and accuracy of patient information are vital for effective treatment and administrative processes. The Patient Summary Form PSF-750, revised on July 1, 2015, serves as a comprehensive document that collects essential data on patients, including personal information, insurance details, and health status. It is designed to streamline the communication between patients, healthcare providers, and insurance companies. This form requires patients to provide specific details such as their name, address, date of birth, insurance ID, health plan, and the referring physician's information if applicable. Instructions included with the form guide patients to complete the submission online within a specified timeframe, ensuring that all information is accurately and promptly provided. It also outlines the necessary information about the billing provider or facility, diagnosis codes, and the nature of the patient's condition, among other clinical details. Moreover, the form includes sections for patient-completed data regarding the onset and intensity of symptoms, their impact on daily activities, and the patient's overall health assessment. This structured approach aims to enhance the efficiency of healthcare delivery by ensuring that all parties have access to accurate and current patient information.
| Question | Answer |
|---|---|
| Form Name | Patient Summary Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | myoptumhealthphysicalhealth patient summary form, humana patient summary form, patient summary form printable, patient summary form |