

In case you desire to fill out determines, there's no need to download any sort of software - just make use of our PDF tool. FormsPal team is continuously working to develop the editor and make it much better for people with its handy features. Benefit from present-day revolutionary prospects, and find a trove of new experiences! Getting underway is easy! All that you should do is follow these basic steps below:
Step 1: Press the "Get Form" button above. It'll open our editor so you can begin completing your form.
Step 2: This tool enables you to change PDF files in a variety of ways. Change it with personalized text, correct what is already in the document, and place in a signature - all possible within minutes!
This document will require some specific details; in order to ensure consistency, you should adhere to the recommendations directly below:
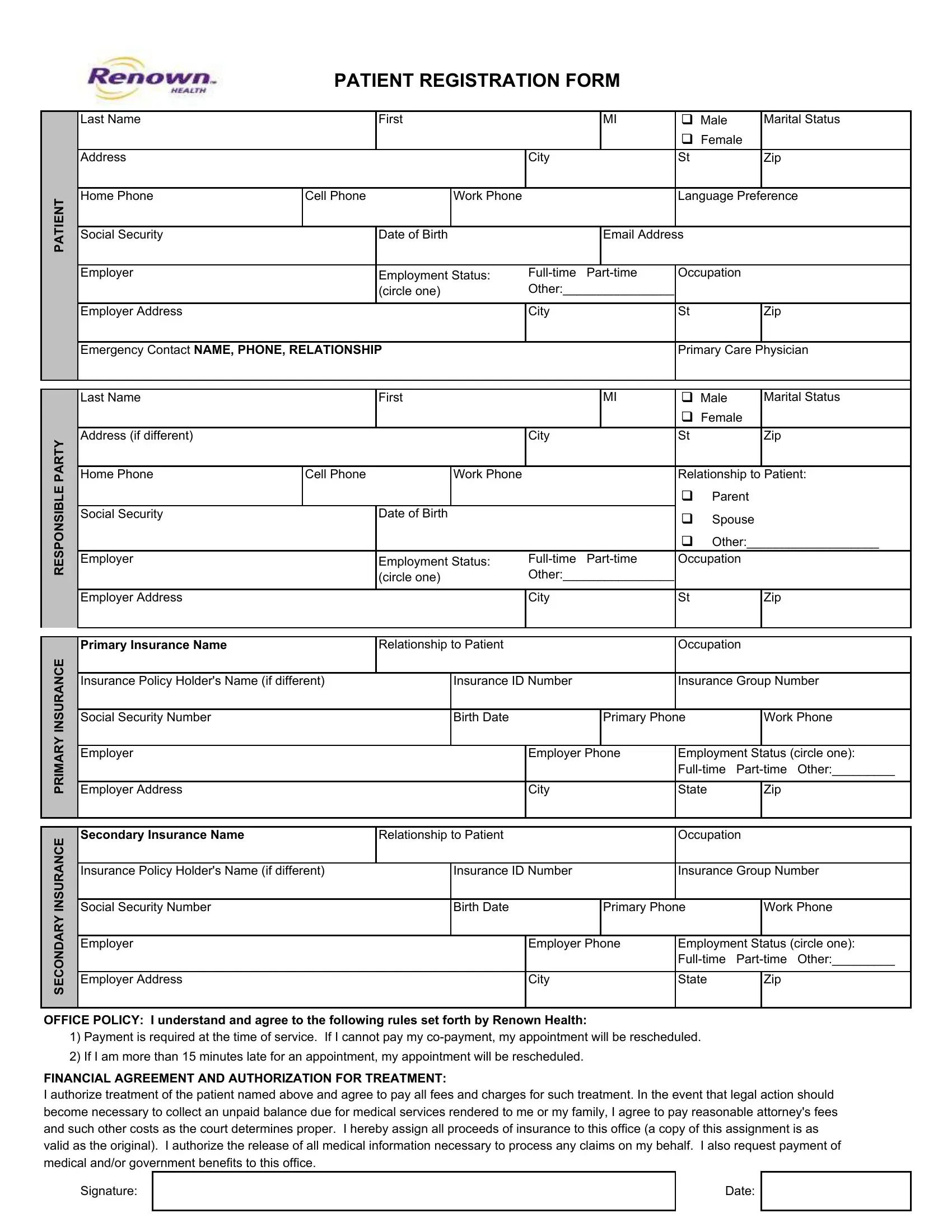
1. It is advisable to complete the determines accurately, hence take care while filling out the parts comprising these particular blank fields:
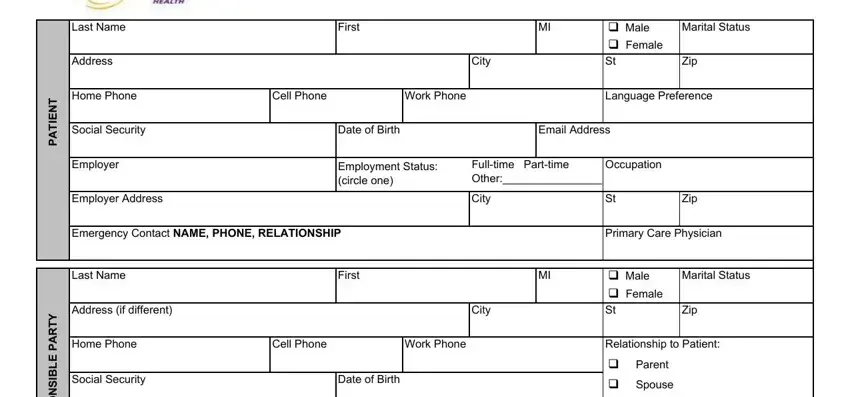
2. The third step is to complete these fields: Relationship to Patient cid Parent, Y T R A P E L B S N O P S E R, Employer, Employer Address, Employment Status circle one, Fulltime Parttime Other, City, Zip, Primary Insurance Name, Relationship to Patient, Occupation, Insurance Policy Holders Name if, Insurance ID Number, Insurance Group Number, and Social Security Number.
Be very attentive when filling out Employer Address and Employer, as this is the section where most users make a few mistakes.
3. In this part, look at FINANCIAL AGREEMENT AND, Signature, and Date. All of these will need to be taken care of with utmost precision.

Step 3: Check the information you've inserted in the form fields and then click the "Done" button. Join us now and easily obtain determines, ready for download. All changes made by you are preserved , meaning you can change the document later on as needed. FormsPal offers risk-free document editing without personal data record-keeping or any sort of sharing. Rest assured that your information is in good hands with us!