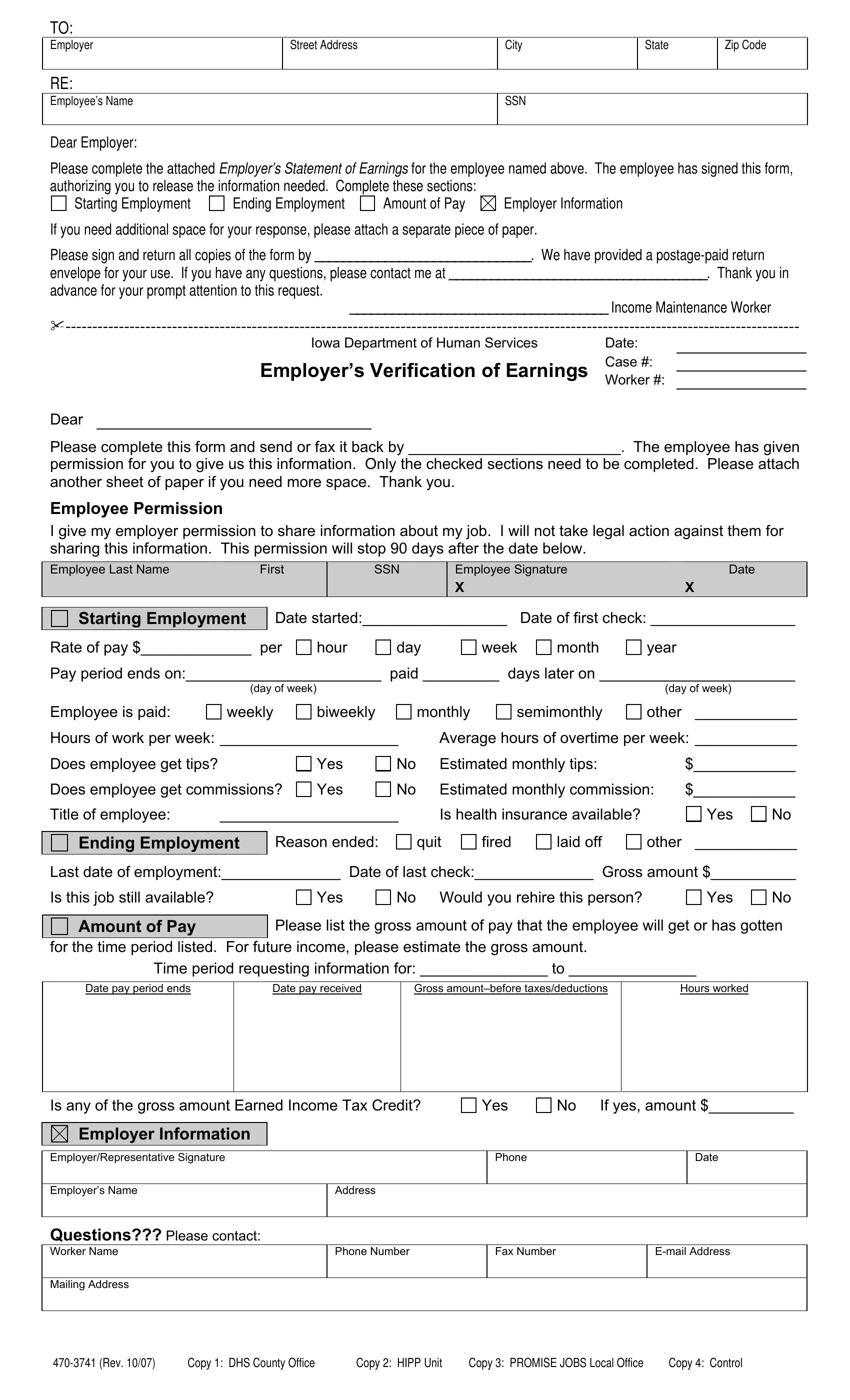
In the multifaceted world of employment and social services, the Employer Verification of Earnings form serves as a vital tool to ensure the accuracy and integrity of financial information provided by employees to various governmental or institutional bodies. Originating from the Iowa Department of Human Services, this document facilitates a structured method for employers to report earnings of their workforce when requested, exemplifying a commitment to transparent and responsible information sharing. Through sections that detail starting and ending employment, amount of pay, and employer specifics, the form encapsulates a comprehensive overview of an individual’s employment journey. Further emphasizing its utility, it includes permissions for the release of this data signed by the employee, thereby safeguarding against legal repercussions and fostering a respectful exchange of personal financial data. Designed to be filled out with ease and returned using a provided postage-paid envelope, the process aims for efficiency and convenience for both parties involved. Moreover, the option to attach additional sheets ensures that complex employment histories can be accommodated without compromise, rounding off a document that is both thorough in its purpose and considerate in its execution.
| Question | Answer |
|---|---|
| Form Name | Employer Verification Of Earnings Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | employment verification of earnings form wisconsin, employer verification of earnings pdf, employment verification form wisconsin, employment verification form pdf wisconsin |
TO:
Employer
RE:
Street Address
City
State
Zip Code
Employee’s Name
SSN
Dear Employer:
Please complete the attached Employer’s Statement of Earnings for the employee named above. The employee has signed this form, authorizing you to release the information needed. Complete these sections:
Starting Employment |
Ending Employment |
Amount of Pay |
Employer Information |
If you need additional space for your response, please attach a separate piece of paper.
Please sign and return all copies of the form by _______________________________. We have provided a
envelope for your use. If you have any questions, please contact me at _____________________________________. Thank you in
advance for your prompt attention to this request.
_____________________________________ Income Maintenance Worker
Iowa Department of Human Services |
Date: |
Employer’s Verification of Earnings |
Case #: |
Worker #: |
Dear
Please complete this form and send or fax it back by _________________________. The employee has given
permission for you to give us this information. Only the checked sections need to be completed. Please attach another sheet of paper if you need more space. Thank you.
Employee Permission
I give my employer permission to share information about my job. I will not take legal action against them for sharing this information. This permission will stop 90 days after the date below.
Employee Last Name |
First |
|
|
SSN
Employee Signature |
Date |
XX
Starting Employment
Date started:_________________ Date of first check: _________________
Rate of pay $_____________ per
hour
day
week
month
year
Pay period ends on:_______________________ paid _________ days later on _______________________
(day of week) |
(day of week) |
Employee is paid:
weekly
biweekly
monthly
semimonthly
other ____________
Hours of work per week: _____________________ |
Average hours of overtime per week: ____________ |
Does employee get tips?
Does employee get commissions?
Yes
Yes
No |
Estimated monthly tips: |
$____________ |
No |
Estimated monthly commission: |
$____________ |
Title of employee: |
_____________________ |
|
|
Reason ended: |
|
Ending Employment |
||
|
|
|
Is health insurance available?
quit |
fired |
laid off |
other |
Yes No
____________
Last date of employment:______________ Date of last check:______________ Gross amount $__________
Is this job still available?
Amount of Pay
Yes |
No Would you rehire this person? |
Yes |
No |
Please list the gross amount of pay that the employee will get or has gotten
for the time period listed. For future income, please estimate the gross amount.
Time period requesting information for: _______________ to _______________
Date pay period ends
Date pay received
Gross
Hours worked
Is any of the gross amount Earned Income Tax Credit?
Yes
No If yes, amount $__________
Employer Information
Employer/Representative Signature |
|
Phone |
Date |
|
|
|
|
Employer’s Name |
Address |
|
|
|
|
|
|
Questions??? Please contact:
Worker Name |
Phone Number |
Fax Number |
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
Copy 1: DHS County Office |
Copy 2: HIPP Unit |
Copy 3: PROMISE JOBS Local Office |
Copy 4: Control |