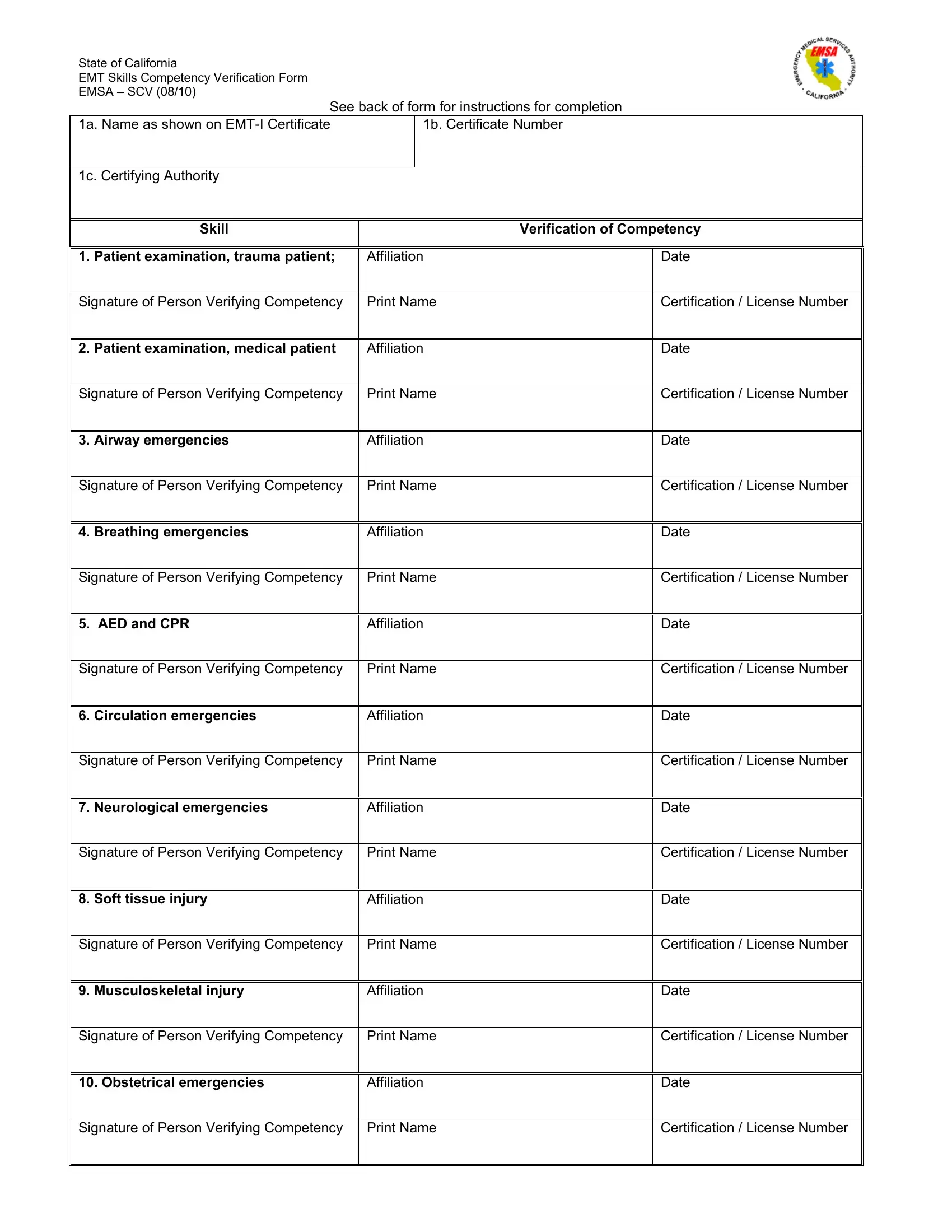
The State of California plays a crucial role in ensuring that Emergency Medical Technicians (EMTs) maintain a high standard of care through continuous verification of their skills. At the heart of this rigorous process is the EMT Skills Competency Verification Form, known as the EMSA – SCV form, which was last updated in August 2010. This comprehensive document serves a pivotal function by meticulously recording the verification of an EMT’s ability to manage a wide range of emergency situations, from trauma and medical patient examinations to specific emergencies involving airway, breathing, and circulation, as well as care for neurological, soft tissue, musculoskeletal, and obstetrical emergencies. Designed for clarity and specificity, the form requires details such as the EMT’s name as it appears on their certificate, certificate number, and the certifying authority, alongside the affiliation, date, and signatory validation of the person verifying competency. The EMSA – SCV form stands not only as a testament to an EMT's current competency in critical skills but also acts as an essential tool in the ongoing effort to improve patient care through professional accountability and development.
| Question | Answer |
|---|---|
| Form Name | Emsa Scv Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | competency verification, emsa verification, california emt skills, skills verification |
State of California
EMT Skills Competency Verification Form
EMSA – SCV (08/10)
See back of form for instructions for completion
1a. Name as shown on |
1b. Certificate Number |
|
|
1c. Certifying Authority |
|
Skill
Verification of Competency
1. |
Patient examination, trauma patient; |
Affiliation |
Date |
|
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|
|
|
2. |
Patient examination, medical patient |
Affiliation |
Date |
|
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|
|
|
3. Airway emergencies |
Affiliation |
Date |
|
|
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|
|
|
4. |
Breathing emergencies |
Affiliation |
Date |
|
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|
|
|
5. |
AED and CPR |
Affiliation |
Date |
|
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|
|
|
6. |
Circulation emergencies |
Affiliation |
Date |
Signature of Person Verifying Competency |
Print Name |
Certification / License Number
7. Neurological emergencies
Affiliation
Date
Signature of Person Verifying Competency |
Print Name |
Certification / License Number
8. Soft tissue injury |
Affiliation |
Date |
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|
9. Musculoskeletal injury |
Affiliation |
Date |
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|
10. Obstetrical emergencies |
Affiliation |
Date |
|
|
|
Signature of Person Verifying Competency |
Print Name |
Certification / License Number |
|
|
|