
medicaid disability application can be completed online effortlessly. Simply make use of FormsPal PDF editor to get the job done without delay. Our editor is constantly evolving to deliver the very best user experience achievable, and that's due to our commitment to continual improvement and listening closely to user opinions. Getting underway is simple! Everything you need to do is adhere to the next easy steps down below:
Step 1: First of all, open the editor by pressing the "Get Form Button" in the top section of this page.
Step 2: Using this online PDF editor, it's possible to accomplish more than just fill out blank form fields. Express yourself and make your forms appear high-quality with custom text added in, or modify the file's original content to perfection - all comes with the capability to incorporate just about any graphics and sign it off.
When it comes to blank fields of this particular PDF, here is what you should consider:
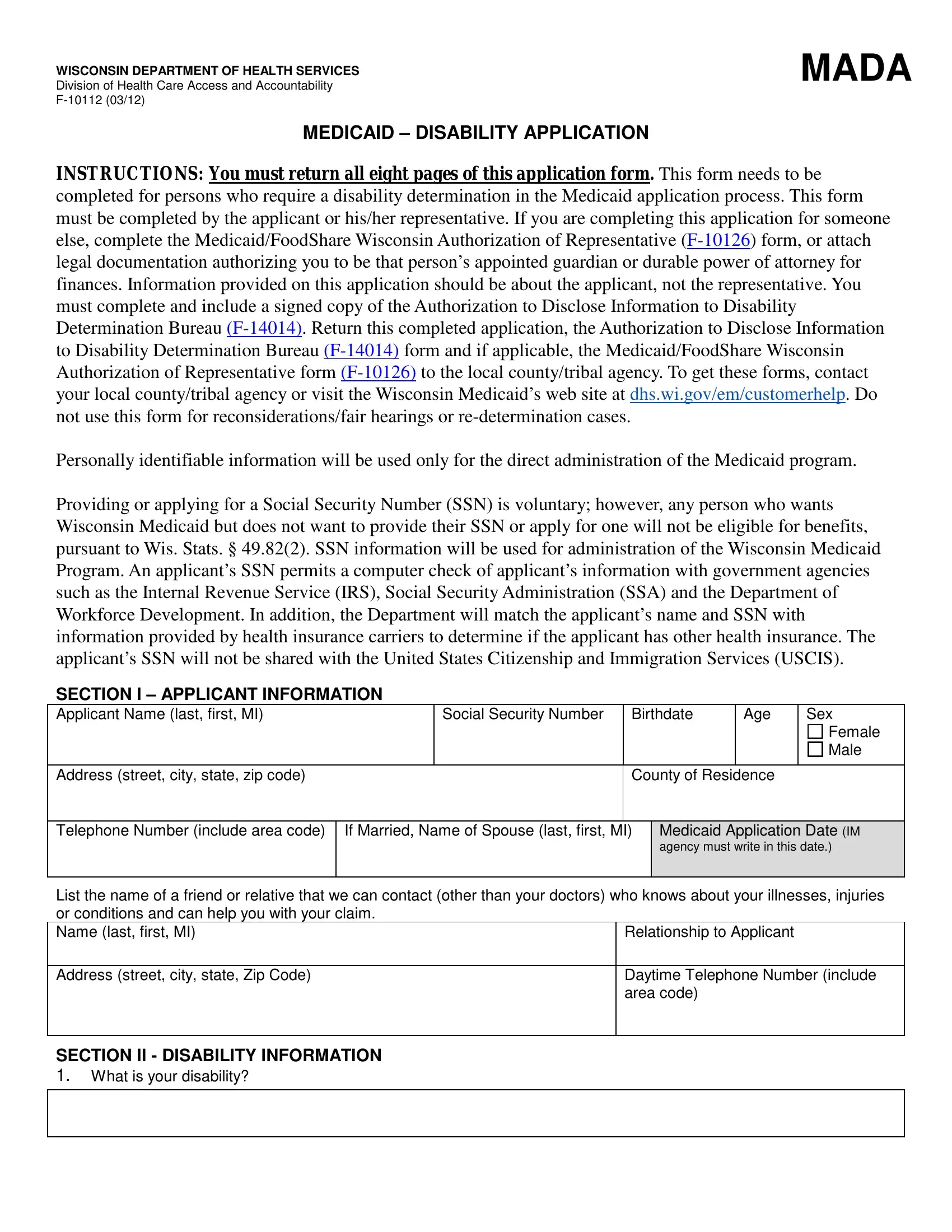
1. You need to complete the medicaid disability application accurately, therefore be attentive when working with the sections containing all of these blanks:
2. Your next stage would be to submit these particular fields: INSTRUCTIONS You must return all, Social Security Number, Birthdate, Age, Sex, Address street city state zip code, Female Male, County of Residence, Telephone Number include area code, If Married Name of Spouse last, agency must write in this date, List the name of a friend or, Relationship to Applicant, Address street city state Zip Code, and SECTION II DISABILITY INFORMATION.
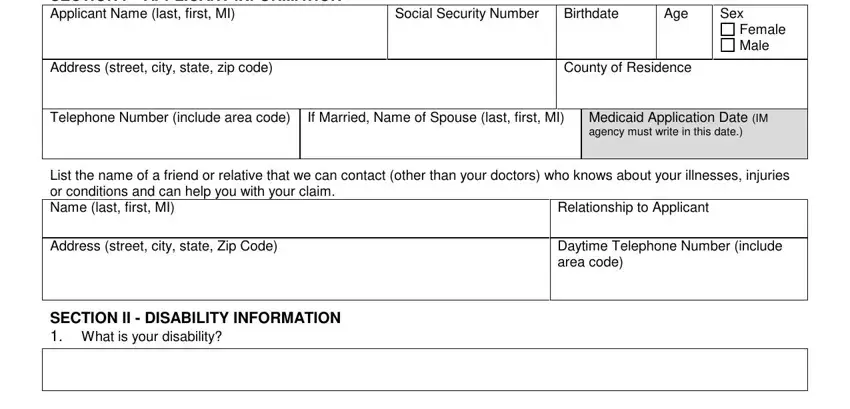
Be really careful while filling in Social Security Number and Address street city state zip code, since this is where a lot of people make errors.
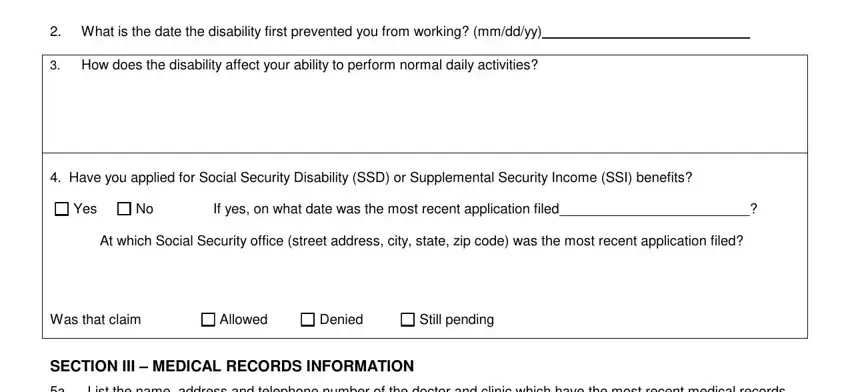
3. Completing What is the date the disability, How does the disability affect, Yes, If yes on what date was the most, Have you applied for Social, Still pending, Allowed, Denied, At which Social Security office, SECTION III MEDICAL RECORDS, and a List the name address and is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. The subsequent paragraph will require your details in the subsequent places: Name of Doctor last first, Business Address street city state, Business Telephone Number include, Clinic Name, How often did you see this doctor, Date you first saw this doctor, Date you last saw this doctor, Reason for the visits, Type of treatment surgery or, b Have you been seen by any other, No If yes list the name address, and Yes. Be sure that you type in all of the needed information to move onward.
5. Now, the following last segment is precisely what you will have to complete before finalizing the form. The blanks in question are the next: MEDICAID DISABILITY APPLICATION F, Business Address street city state, Business Telephone Number include, How often did you see this doctor, Date the applicant first saw this, Date the applicant last saw this, Reason for the visits, Type of treatment surgery or, Name of Doctor last first, Business Address street city state, and Business Telephone Number include.
Step 3: After you have looked again at the details in the document, just click "Done" to conclude your form at FormsPal. Make a 7-day free trial option with us and gain instant access to medicaid disability application - download, email, or change in your personal account page. We do not share or sell any details you enter whenever dealing with forms at our site.