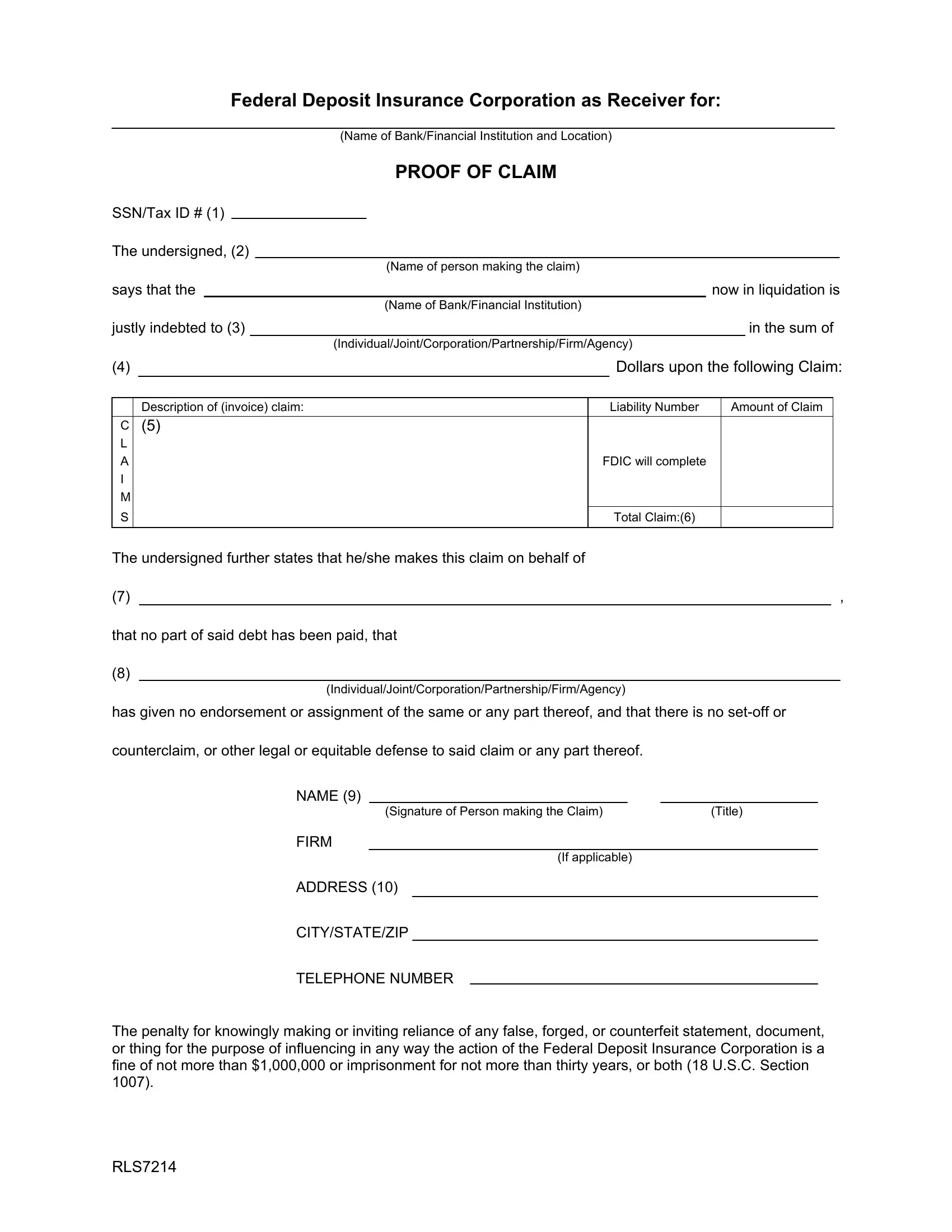
When a bank or financial institution fails, the Federal Deposit Insurance Corporation (FDIC) steps in to manage the liquidation and ensure creditors are fairly compensated for their losses. The FDIC Proof of Claim form serves as a critical tool in this process, allowing individuals and entities to officially submit their claims against the failed institution. The form requires detailed information, including the claimant's name, the amount owed, and a comprehensive description of the claim, to be submitted for evaluation. Furthermore, it emphasizes the importance of honesty, warning of severe penalties for false claims. Completing this form correctly is essential for claimants, as it is the primary means through which they can hope to recover funds or assets lost due to the institution's failure. Along with detailed instructions, the form also specifies the required documentation to support claims for goods purchased or services rendered, ensuring that the FDIC has all necessary information to accurately assess and address each claim.
| Question | Answer |
|---|---|
| Form Name | Fdic Proof Of Claim Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | federal deposit proof of, how to fdic of claim, deposit proof claim, fdic insurance of claim |
Federal Deposit Insurance Corporation as Receiver for:
|
|
|
|
|
|
|
(Name of Bank/Financial Institution and Location) |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
PROOF OF CLAIM |
|
|
|
|
|
|
|||
SSN/Tax ID # (1) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
The undersigned, (2) |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
(Name of person making the claim) |
|
|
|
|
|
|
|||
says that the |
|
|
|
|
|
|
now in liquidation is |
||||||||||
|
|
|
|
|
|
|
|
(Name of Bank/Financial Institution) |
|
|
|
|
|
|
|||
justly indebted to (3) |
|
|
|
|
|
|
|
in the sum of |
|||||||||
|
|
|
|
|
|
|
(Individual/Joint/Corporation/Partnership/Firm/Agency) |
|
|
|
|
|
|
||||
(4) |
|
|
|
|
|
|
|
|
|
Dollars upon the following Claim: |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Description of (invoice) claim: |
|
|
|
Liability Number |
|
Amount of Claim |
|
|
|||||||
C |
(5) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
FDIC will complete |
|
|
|
|
|
|
||
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
Total Claim:(6) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The undersigned further states that he/she makes this claim on behalf of |
|
|
|
|
|
|
|||||||||||
(7) |
|
|
|
|
|
|
|
|
|
|
|
|
, |
||||
that no part of said debt has been paid, that
(8)
(Individual/Joint/Corporation/Partnership/Firm/Agency)
has given no endorsement or assignment of the same or any part thereof, and that there is no
counterclaim, or other legal or equitable defense to said claim or any part thereof.
NAME (9)
(Signature of Person making the Claim) |
(Title) |
FIRM
(If applicable)
ADDRESS (10)
CITY/STATE/ZIP
TELEPHONE NUMBER
The penalty for knowingly making or inviting reliance of any false, forged, or counterfeit statement, document, or thing for the purpose of influencing in any way the action of the Federal Deposit Insurance Corporation is a fine of not more than $1,000,000 or imprisonment for not more than thirty years, or both (18 U.S.C. Section 1007).
RLS7214
GENERAL INFORMATION AND INSTRUCTIONS FOR
COMPLETING A PROOF OF CLAIM FORM
This form is being sent to you in the event you believe the failed institution owes you funds for services rendered or goods purchased prior to the date of closing. If the institution does not currently owe you any money, it is not necessary for you to complete this form.
The following blanks must be completed in order for your Proof of Claim to be considered: (The numbers correspond with those located on the proof of claim form.)
1)A company's tax identification number or an individual's social security number.
2)Name of the person making the claim.
3)Review this name. Make corrections as needed. Fill in name if blank.
4)Written dollar amount of the claim (ex. One hundred and no/100.)
5)Detailed description of what is being claimed (i.e., the invoice number, type of service being claimed, account number, etc.).
6)Total amount of claim. Total should NOT include interest or late fees accrued since institution closing.
7)Review this name. Make corrections as needed. Fill in name if blank.
8)Review this name. Make corrections as needed. Fill in name if blank.
9)Signature of the person making claim and the title of that person if they are representing a company making a claim.
10)The address and telephone number of the individual or company making the claim.
Should the above information be missing, your information will be entered into our tracking system, but your Proof of Claim form will be returned to you for completion.
REQUIRED DOCUMENTATION
1)Claims for Goods Purchased by the Former Institution: You must forward a copy of the Purchase order or other correspondence from the institution requesting the goods, a copy of your invoice and a receipt signed by the institution indicating that the goods were received.
2)Claims for Services Rendered: You must forward a copy of the correspondence or signed initial contract sent by the institution to request your services and an invoice. In the case of legal fees, an itemized invoice must be sent indicating your prorated charges. For appraisal services, submit proof the appraisal was completed.
RLS7214 |
2 |