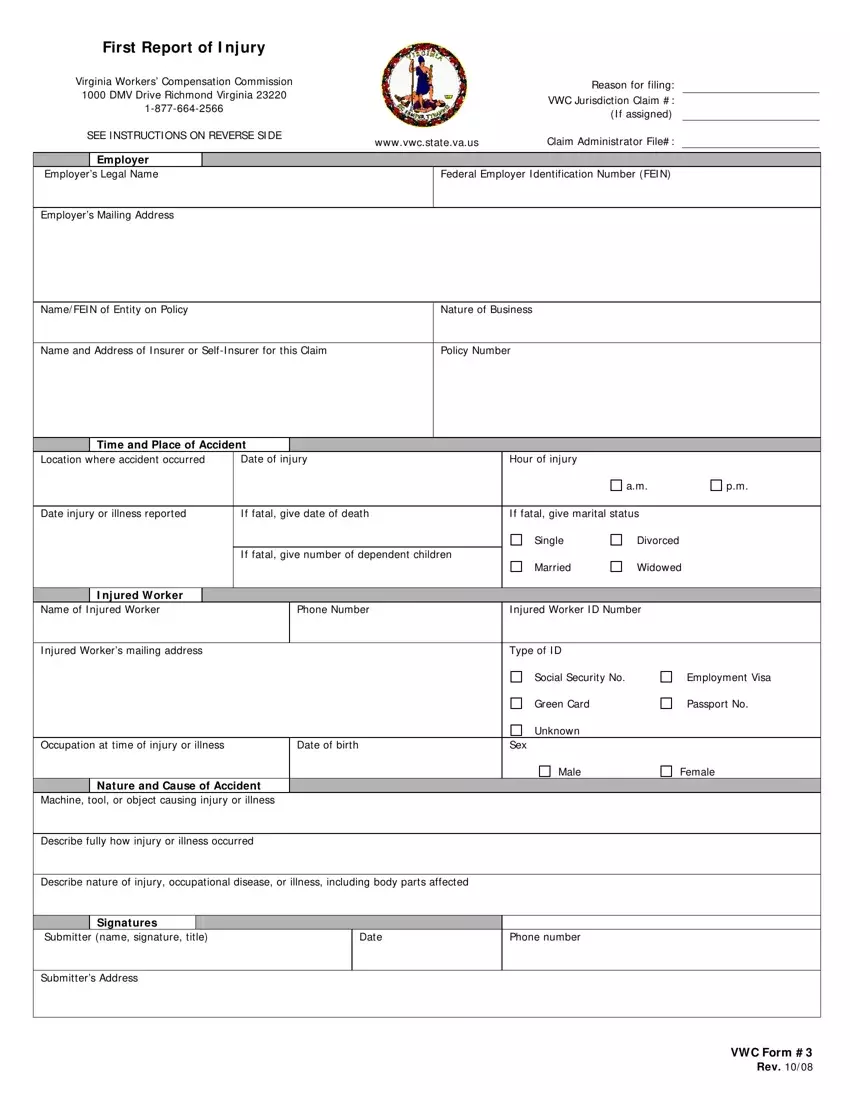
Filing the First Report of Injury (VWC Form #3) is the first step in initiating a workers' compensation claim for a workplace injury. Below is a step-by-step guide on how to properly fill out this document.
1. Employer Information
Write the employer’s legal name and Federal Employer Identification Number (FEIN). Provide the employer's mailing address. Next, input the name and FEIN of the entity on the insurance policy and specify the nature of the business.
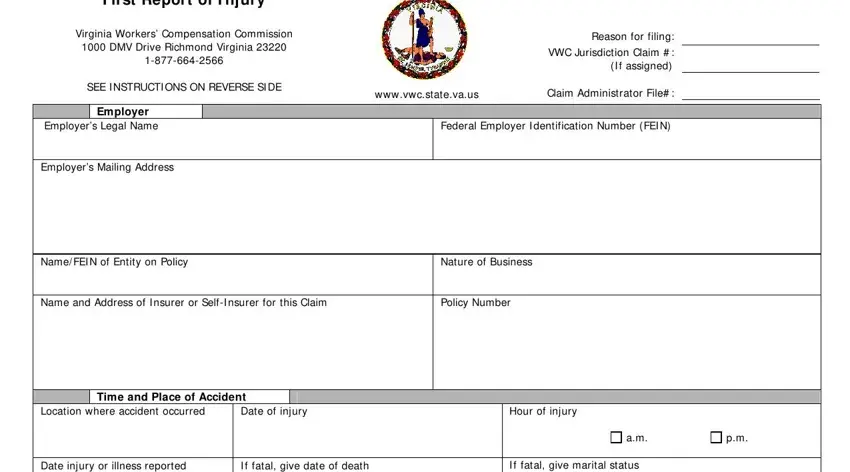
2. Insurer or Self-Insurer Details
Fill in the name and address of the insurer or self-insurer responsible for this claim. Record the policy number related to this specific workers’ compensation coverage.
3. Accident Details
Record the location where the accident occurred, followed by the exact date and hour of the injury. If the injury was fatal, provide the date of death.
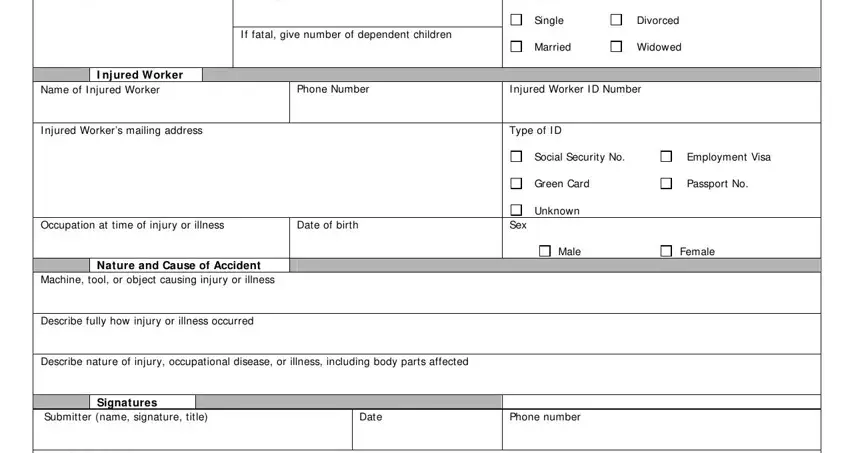
4. Report Injury or Illness
Detail the date the injury or illness was reported to the employer. If the injury resulted in death, include the number of dependent children and the marital status of the deceased at the time of death.
5. Injured Worker Details
Enter the injured worker's name, phone number, and ID number. Specify the type of ID provided, whether it’s a Social Security Number, Employment Visa, Green Card, or Passport Number. Include the injured worker’s mailing address, occupation at the time of injury or illness, date of birth, and sex.
6. Accident and Injury Description
Fully describe how the injury or illness occurred, including any machines, tools, or objects involved. Detail the nature of the injury or occupational disease, specifically noting affected body parts.

7. Signature and Submission
The form should be signed and dated by the person preparing it, typically the employer or an HR representative. Provide the submitter's name, phone number, and address. After completing the form, send it to the claim administrator for the insurance company, who will then handle its submission to the Virginia Workers’ Compensation Commission.
