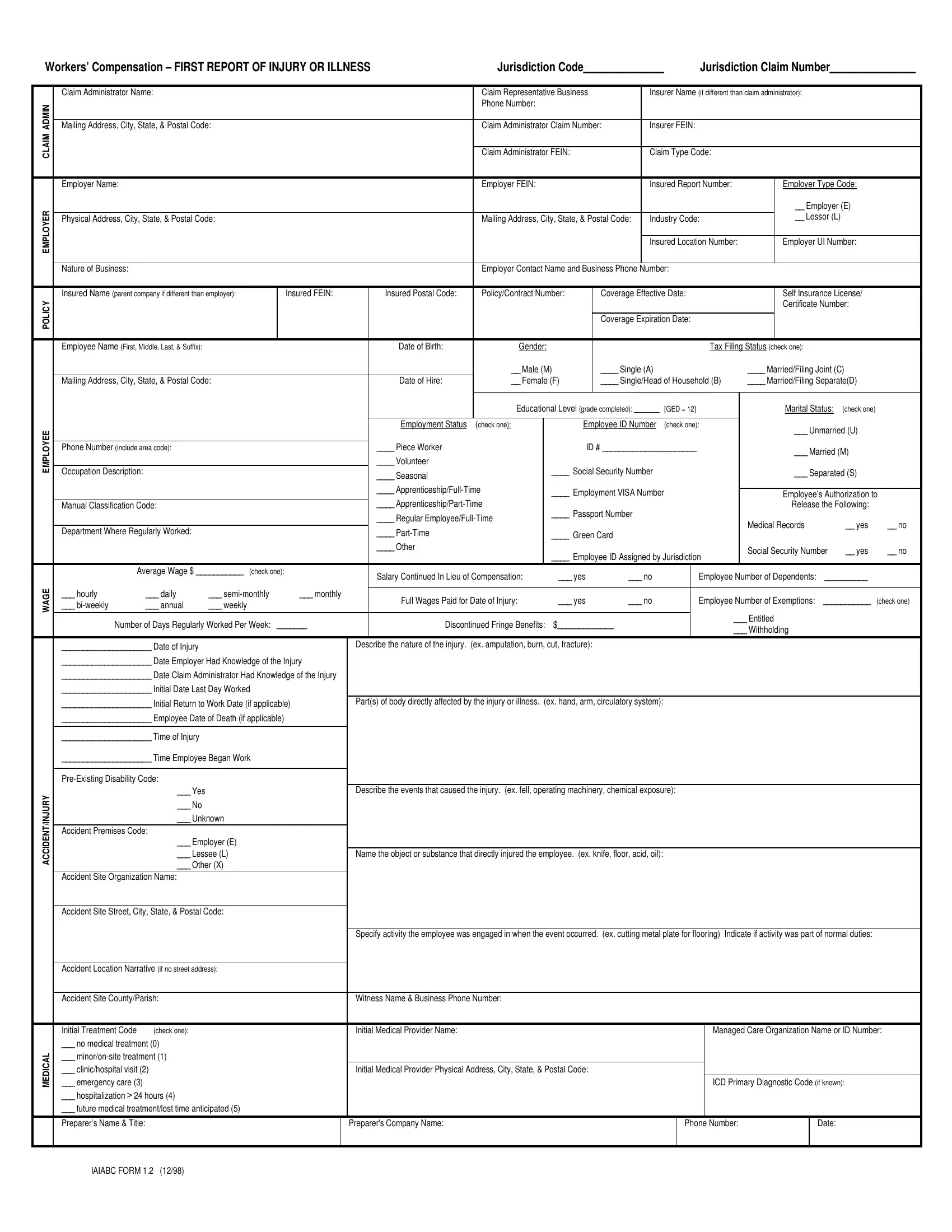
When an employee gets injured or falls ill due to their work, the First Report of Injury or Illness form becomes a critical document for starting the process of a workers' compensation claim. This form is not just a mere procedural requirement; it plays a pivotal role in ensuring that employees receive the benefits and support they need during their recovery period. It gathers comprehensive details about the injured or ill employee, including personal information, employment data, and the specifics of the injury or illness incurred. This form also outlines the nature of the business, the employer's information, and details about the insurance coverage, all of which are essential for processing the claim effectively. Moreover, the information provided about the accident or illness—such as the time, date, and how the event occurred—helps determine the legitimacy of the claim and the extent of compensation the employee is entitled to. Accurately and promptly filling out this form not only facilitates a smoother claim process but also ensures that the employee receives the appropriate medical care and compensation in a timely manner, reinforcing the safety net that workers' compensation provides.
| Question | Answer |
|---|---|
| Form Name | First Report Of Injury Or Illness Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | iowa workers' compensation first report of injury form, first report injury, iowa first report injury, first report of injury iowa 2018 |
Workers’ Compensation – FIRST REPORT OF INJURY OR ILLNESS |
Jurisdiction Code______________ |
|
|
Jurisdiction Claim Number_______________ |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Claim Administrator Name: |
|
|
|
|
|
|
Claim Representative Business |
|
Insurer Name (if different than claim administrator): |
|
|
|
|||||||||||
ADMIN |
|
|
|
|
|
|
|
|
Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Mailing Address, City, State, & Postal Code: |
|
|
|
|
|
Claim Administrator Claim Number: |
Insurer FEIN: |
|
|
|
|
|
|
|||||||||||
CLAIM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Claim Administrator FEIN: |
|
Claim Type Code: |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Employer Name: |
|
|
|
|
|
|
|
Employer FEIN: |
|
|
|
Insured Report Number: |
|
Employer Type Code: |
|
||||||||
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__ Employer (E) |
|
|||
|
Physical Address, City, State, & Postal Code: |
|
|
|
|
|
Mailing Address, City, State, & Postal Code: |
Industry Code: |
|
__ Lessor (L) |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insured Location Number: |
|
Employer UI Number: |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Nature of Business: |
|
|
|
|
|
|
|
Employer Contact Name and Business Phone Number: |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Insured Name (parent company if different than employer): |
|
Insured FEIN: |
|
Insured Postal Code: |
Policy/Contract Number: |
Coverage Effective Date: |
|
Self Insurance License/ |
|
||||||||||||||
POLICY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Certificate Number: |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Coverage Expiration Date: |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee Name (First, Middle, Last, & Suffix): |
|
|
|
|
|
Date of Birth: |
Gender: |
|
|
|
|
|
|
|
Tax Filing Status (check one): |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
__ Male (M) |
____ Single (A) |
|
|
|
|
____ Married/Filing Joint (C) |
|
||||||||
|
Mailing Address, City, State, & Postal Code: |
|
|
|
|
Date of Hire: |
__ Female (F) |
____ Single/Head of Household (B) |
____ Married/Filing Separate(D) |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Educational Level (grade completed): _______ |
[GED = 12] |
|
Marital Status: |
(check one) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
EMPLOYEE |
|
|
|
|
|
|
|
Employment Status |
(check one): |
|
|
Employee ID Number |
(check one): |
|
___ Unmarried (U) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone Number (include area code): |
|
|
|
|
|
____ Piece Worker |
|
|
|
ID # ______________________ |
|
___ Married (M) |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
____ Volunteer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupation Description: |
|
|
|
|
|
|
____ Seasonal |
|
|
____ Social Security Number |
|
|
|
|
|
___ Separated (S) |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____ |
|
____ Employment VISA Number |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee’s Authorization to |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Manual Classification Code: |
|
|
|
|
|
____ |
|
____ Passport Number |
|
|
|
|
|
|
Release the Following: |
|
|||||||
|
|
|
|
|
|
|
|
____ Regular |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical Records |
|
__ yes |
__ no |
||||
|
Department Where Regularly Worked: |
|
|
|
|
|
____ |
|
|
____ Green Card |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
____ Other |
|
|
|
|
|
|
|
|
|
|
Social Security Number |
__ yes |
__ no |
|||
|
|
|
|
|
|
|
|
|
|
|
____ Employee ID Assigned by Jurisdiction |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Average Wage $ ___________ (check one): |
|
Salary Continued In Lieu of Compensation: |
|
___ yes |
___ no |
|
|
Employee Number of Dependents: |
__________ |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
WAGE |
___ hourly |
___ daily |
___ |
|
___ monthly |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Full Wages Paid for Date of Injury: |
|
___ yes |
___ no |
|
|
Employee Number of Exemptions: |
___________ |
(check one) |
||||||||||||||
|
___ |
___ annual |
___ weekly |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Entitled |
|
|
|
|||
|
Number of Days Regularly Worked Per Week: |
_______ |
|
|
Discontinued Fringe Benefits: |
$_____________ |
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
___ Withholding |
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
_____________________ Date of Injury |
|
|
|
|
Describe the nature of the injury. (ex. amputation, burn, cut, fracture): |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
_____________________ Date Employer Had Knowledge of the Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
_____________________ Date Claim Administrator Had Knowledge of the Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
_____________________ Initial Date Last Day Worked |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
_____________________ Initial Return to Work Date (if applicable) |
Part(s) of body directly affected by the injury or illness. (ex. hand, arm, circulatory system): |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
_____________________ Employee Date of Death (if applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____________________ Time of Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____________________ Time Employee Began Work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
ACCIDENT/INJURY |
|
___ Yes |
|
|
|
|
Describe the events that caused the injury. (ex. fell, operating machinery, chemical exposure): |
|
|
|
|
|
|
|||||||||||
|
___ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Premises Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Employer (E) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Lessee (L) |
|
|
|
Name the object or substance that directly injured the employee. (ex. knife, floor, acid, oil): |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
___ Other (X) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Site Organization Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Accident Site Street, City, State, & Postal Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
Specify activity the employee was engaged in when the event occurred. (ex. cutting metal plate for flooring) Indicate if activity was part of normal duties: |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Accident Location Narrative (if no street address): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Accident Site County/Parish: |
|
|
|
|
Witness Name & Business Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Initial Treatment Code |
(check one): |
|
|
|
|
Initial Medical Provider Name: |
|
|
|
|
|
|
|
|
|
Managed Care Organization Name or ID Number: |
|||||||
|
___ no medical treatment (0) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL |
___ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ emergency care (3) |
|
|
|
|
|
Initial Medical Provider Physical Address, City, State, & Postal Code: |
|
|
|
|
|
ICD Primary Diagnostic Code (if known): |
|
|||||||||||
|
___ clinic/hospital visit (2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
___ hospitalization > 24 hours (4) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ future medical treatment/lost time anticipated (5) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Preparer’s Name & Title: |
|
|
|
|
|
Preparer's Company Name: |
|
|
|
|
|
|
|
Phone Number: |
|
|
|
Date: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IAIABC FORM 1.2 (12/98)
Mail to: DIVISION OF WORKERS' COMPENSATION |
STATE OF IOWA |
DIVISION OF LABOR SERVICES |
|
1000 E GRAND |
EMPLOYERS WORK INJURY REPORT |
1000 E GRAND |
|
DES MOINES, IOWA 50319 |
EMPLOYERS FIRST REPORT OF INJURY |
DES MOINES, IOWA 50319 |
|
|
|
||
This section is to provide information valuable in handling this claim.
The Iowa Occupational Safety and Health Act
The following is a summary of the recordkeeping, reporting and posting responsibilities of employers under Iowa’s Occupational Safety and Health Act.
RECORDKEEPING REQUIREMENTS
Regulations issued under the Iowa Occupational Safety and Health Act of 1972 require establishments subject to the Act to maintain records of recordable occupational injuries and illness. Such records must consist of: (a) a log and summary of occupational injuries and illnesses and (b) a supplementary record of each occupational injury and illness.
LOG AND SUMMARY OF OCCUPATIONAL INJURIES AND ILLNESSES. Each recordable occupational injury and occupational illness must be entered on a log and summary of cases (0SHA Form No. 200) as early as practicable but no later than 6 working days after receiving information that a recordable case has occurred. A
SUPPLEMENTARY RECORD OF OCCUPATIONAL INJURIES AND ILLNESSES. To supplement the Log and Summary of Occupational Injuries and Illnesses, each employer must have available a record for each occupational injury or illness at each establishment within 6 working days after receiving information that a recordable case has occurred, OSHA Form No. 101 may be used for this purpose. State of Iowa Form No
ANNUAL SUMMARY. Each employer subject to the recordkeeping requirements must prepare a summary of the occupational injury and illness experience of the employees in each of the employer’s establishments at the end of each year based on the information contained in the log and summary of occupational injuries and illnesses for the particular establishment. OSHA Form No. 200 shall be used for this purpose. The summary shall be signed and posted in a place accessible to the employees no later than February 1 and shall remain in place until March 1. For employees who do not report to work at a single establishment, or who do not report to any fixed establishment on a regular basis, employers shall satisfy the posting requirement by presenting or mailing a copy of the annual summary during the month of February to all such employees who receive pay during that month. Summaries must be retained for 5 years following the end of the calendar year to which they relate.
EMPLOYEES NOT IN FIXED ESTABLISHMENTS. Employers of employees engaged in physically dispersed operations such as occur in construction, installation, repair or service activities who do not report to any fixed establishment on a regular basis but are subject to common supervision may satisfy the recordkeeping provisions with respect to such employees by:
(a)Maintaining the required records for each operation or group of operations which is subject to common supervision (field superintendent, field supervision, etc.) in an established central place;
(b)Having the address and telephone number of the central place available at each worksite; and
(c)Having personnel available at the central place during normal business hours to provide information from the records maintained there by telephone and by mail.
(Note: This regulation does not automatically apply to all construction, installation, repair or service activities. If in doubt about applicability to your operations, contact the Iowa Division of Labor Services.)
Records for personnel who do not primarily report or work at a single establishment, and who are generally not supervised in their daily work, such as traveling salespersons, technicians, engineers, etc., shall be maintained at the location from which they are paid or the base from which personnel operate to carry out their activities.
REPORTING REQUIREMENTS
Regulations issued under the Iowa Occupational Safety and Health Act require all employers subject to the Act to report in writing to the Iowa Workers' Compensation Commissioner any occupational injury or illness which temporarily disables an employee for more than three days or which results in permanent total disability, permanent partial disability, or death. State of Iowa Form No.
Iowa Division of Workers' Compensation shall forward all such reports to the Iowa Division of Labor Services.
In addition, employers must report to the Iowa Labor Commissioner within 8 hours each accident or health hazard that results in one or more fatalities or hospitalization of three or more employees. The toll free number that is available 24 hours a day, including weekends and holidays, to use to report is
Those establishments selected to participate in the annual Occupational Injuries and Illnesses Survey will be required to prepare a report (OSHA Form No
POSTING REQUIREMENTS
The Iowa Occupational Safety and Health Act requires that employees be informed of the job safety and health protection provided under the Act. The poster, “Safety and Health Protection on the Job,” is to be used for this purpose, and must be posted in a prominent place in the establishment to which the employees usually report to work. The poster briefly states the intent and coverage of the Act and the responsibilities of employers and employees to maintain safe and healthful working conditions.
EMPLOYERS WHO MUST KEEP OSHA RECORDS
Employers with 11 or more employees (at any one time in the previous calendar year) in the following industries must keep OSHA records. The industries are identified by name and by the appropriate Standard Industrial Classification (SIC) code:
•Agriculture, forestry, and fishing (SIC’s
•Oil and gas extraction (SIC 13 and 1477)
•Construction (SIC’s
•Manufacturing (SIC’s
•Transportation and public utilities (SIC’s
•Wholesale trade (SIC’s
•Building materials and garden supplies (SIC 52)
•General merchandise and food stores (SIC’s 53 and 54)
•Hotels and other lodging places (SIC 70)
•Repair services (SIC’s 75 and 76)
•Amusement and recreation services (SIC 79)
•Health services (SIC 80), and
•State and local government (Above SIC ‘s plus
If employers in any of the industries listed above have more than one establishment with combined employment of 11 or more employees, records must be kept for each individual establishment.
All employers, including small employers and those in exempted SIC’s, must continue to meet the requirement to report fatalities or multiple (3 or more) hospitalizations and all occupational injuries or occupational illnesses that result in a workers' compensation case.
If an employer is notified in writing by the Bureau of Labor Statistics about having been selected to participate in a statistical survey, such employer, including small employers, and those in exempted SIC’s, must maintain a log and summary of all occupational injuries and illnesses for that year. The notification will contain the necessary form and instructions to comply with the survey requirements.
The Iowa Workers’ Compensation Act
The following is a summary of the recordkeeping and reporting responsibilities of employers under the Iowa Workers’ Compensation Act.
RECORDS AND REPORTS
Every employer shall keep a record of all injuries sustained by employees in the course of their employment resulting in incapacity for longer than one day. An employer with notice or knowledge of an injury which temporarily disables an employee for more than three (3) days or results in permanent total disability, permanent partial disability or death is required to file a report with the Workers' Compensation Commissioner, on State of Iowa Form No.
All books, records and payrolls of an employer are required to be open for inspection by the Workers' Compensation Commissioner for purposes of administration of the Iowa Workers’ Compensation Act.
The Workers' Compensation Commissioner may require an employer to appear and show cause why the employer should not be subject to a civil penalty of $100.00 per occurrence for failure to comply with the reporting or inspection requirements. Upon hearing, if the facts indicate, the commissioner may enter an order requiring payment of such penalty. Unless voluntarily paid, the commissioner may petition the district court for entry of judgment on the order. The employer’s insurance carrier shall be responsible in the same manner and to the same extent as the employer when a report of injury has been submitted to the employer’s insurance carrier and not filed by them with the Workers' Compensation Commissioner.
The employer is required to furnish to an employee, on request, one statement of earnings, wages or salary for the year preceding the injury. An employer may be subject to a civil penalty of $25.00 per offense for refusal to furnish such wage statement.
INSTRUCTIONS
An employer with notice or knowledge of an injury which temporarily disables an employee for more than THREE (3) days or results in permanent total disability, permanent partial disability or death is required to file a copy of this report with the Iowa DIVISION OF WORKERS' COMPENSATION within FOUR (4) days from such event when such injury is alleged by the employee to have been sustained in the course of the employee’s employment. A report to the Iowa DIVISION OF WORKERS' COMPENSATION is considered to also be a report to the Iowa DIVISION OF LABOR SERVICES. The Iowa DIVISION OF WORKERS' COMPENSATION shall forward this report to the Iowa Division of Labor Services. Employers should also report ALL injuries to their insurance carrier. ALL REPORTS MUST BE FILLED IN COMPLETELY AND
SIGNED. PLEASE TYPE OR PRINT LEGIBLY.
This form contains all items requested on OSHA form No 101, “Supplementary Record of Occupational Injuries and Illness.”
THE INFORMATION PROVIDED WILL BE OPEN FOR PUBLIC INSPECTION UNDER Iowa Code § 22.11.
Iowa Form