 No
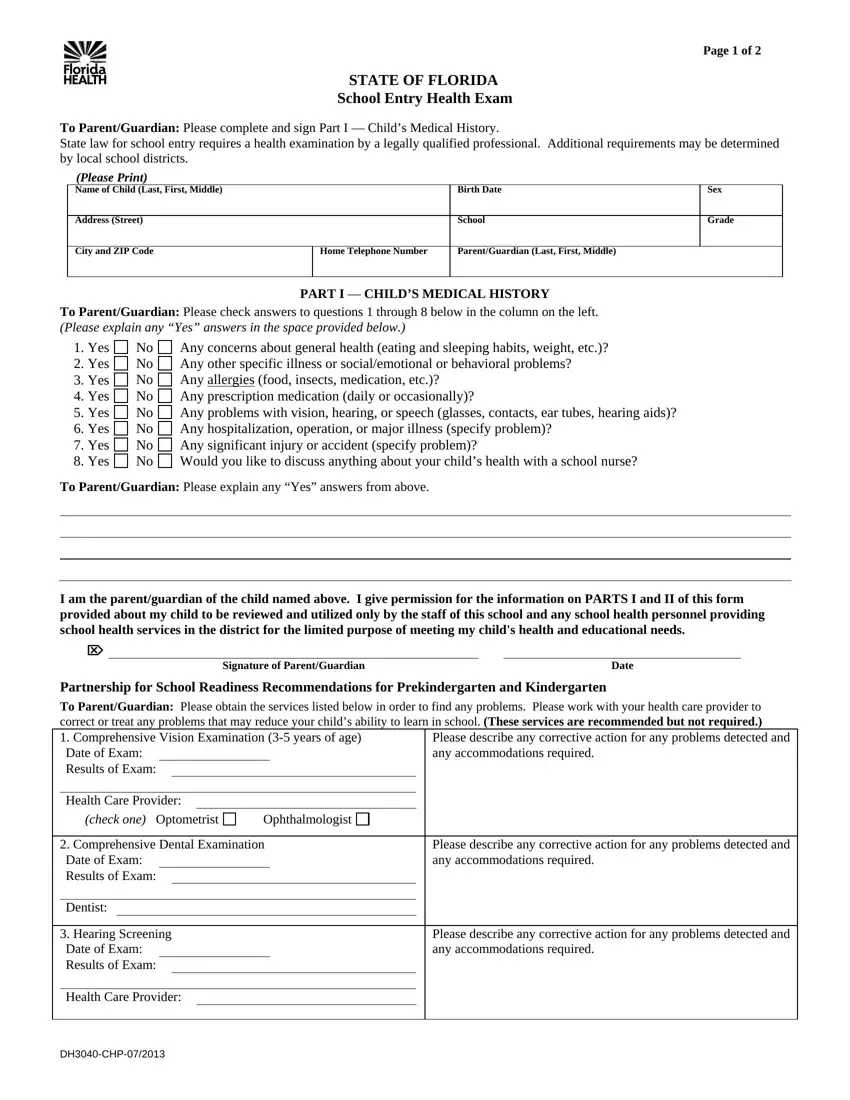
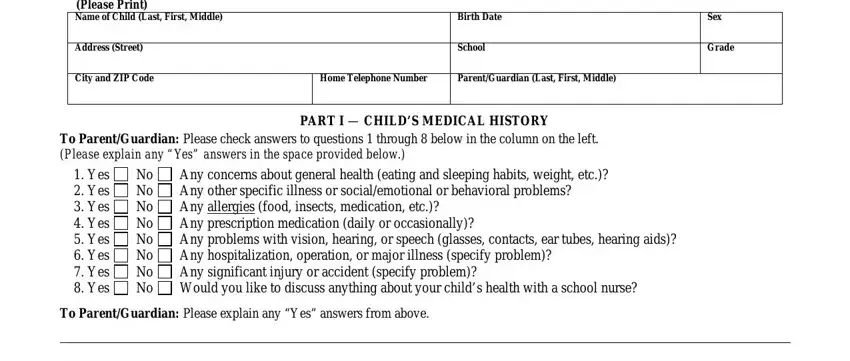
No  Any concerns about general health (eating and sleeping habits, weight, etc.)?
Any concerns about general health (eating and sleeping habits, weight, etc.)? No
No  Any other specific illness or social/emotional or behavioral problems?
Any other specific illness or social/emotional or behavioral problems? No
No  Any
Any  No
No  Any prescription medication (daily or occasionally)?
Any prescription medication (daily or occasionally)? No
No  Any problems with vision, hearing, or speech (glasses, contacts, ear tubes, hearing aids)?
Any problems with vision, hearing, or speech (glasses, contacts, ear tubes, hearing aids)? No
No  Any hospitalization, operation, or major illness (specify problem)?
Any hospitalization, operation, or major illness (specify problem)? No
No  Any significant injury or accident (specify problem)?
Any significant injury or accident (specify problem)? No
No  Would you like to discuss anything about your child’s health with a school nurse?
Would you like to discuss anything about your child’s health with a school nurse?
 This child may participate in school activities including physical education with the following restriction/adaptation. (Specify reason and restriction)
This child may participate in school activities including physical education with the following restriction/adaptation. (Specify reason and restriction)This PDF editor was made to be as easy as possible. While you stick to the following actions, the procedure for filling in the form dh 3040 form will undoubtedly be effortless.
Step 1: Discover the button "Get Form Here" and press it.
Step 2: At the moment you're on the form editing page. You may modify and add content to the document, highlight specified content, cross or check certain words, insert images, put a signature on it, erase unwanted fields, or remove them altogether.
If you want to fill out the form, provide the information the application will require you to for each of the next sections:
The software will expect you to complete the I am the parentguardian of the, Signature of ParentGuardian, Date, Partnership for School Readiness, Please describe any corrective, Health Care Provider, check one Optometrist, Ophthalmologist, Comprehensive Dental Examination, Dentist, and Please describe any corrective field.
The system will ask you for information to conveniently submit the box Hearing Screening Date of Exam, Health Care Provider, DHCHP, and Please describe any corrective.
For field Name of Child Last First Middle, School Entry Health Exam Page of, Birth Date, To be completed and signed by the, PART II MEDICAL EVALUATION, Exam must be within one year of, Month, Day, Year, Screening Results, Height, Weight, BMI, HctHgb, and Lead, specify the rights and responsibilities.

Finish by taking a look at all these areas and preparing them accordingly: This child has a health condition, This form will be stored in the, Recommendations Attach additional, Please Check One, This child may participate fully, Specify reason and restriction, SignatureTitle of Health Care, Date, Address Please print or stamp, Name Please print or stamp, and Tuberculosis Targeted Testing.
Step 3: Hit the "Done" button. Now you may export the PDF document to your device. Besides, you may send it via email.
Step 4: Prepare a duplicate of any document. It would save you time and make it easier to remain away from complications in the future. Also, your data will not be revealed or monitored by us.
