Schools and childcare programs require the DH 680 form before children entering classes can begin attending. Staff follow FLDOH Immunization Requirements and use the form to verify that each student meets state health standards. Usually, parents or a guardian receive this record from enrolled health care providers or the County Health Department. They must then submit the form when their child joins a licensed childcare facility, family daycare home, or begins kindergarten.
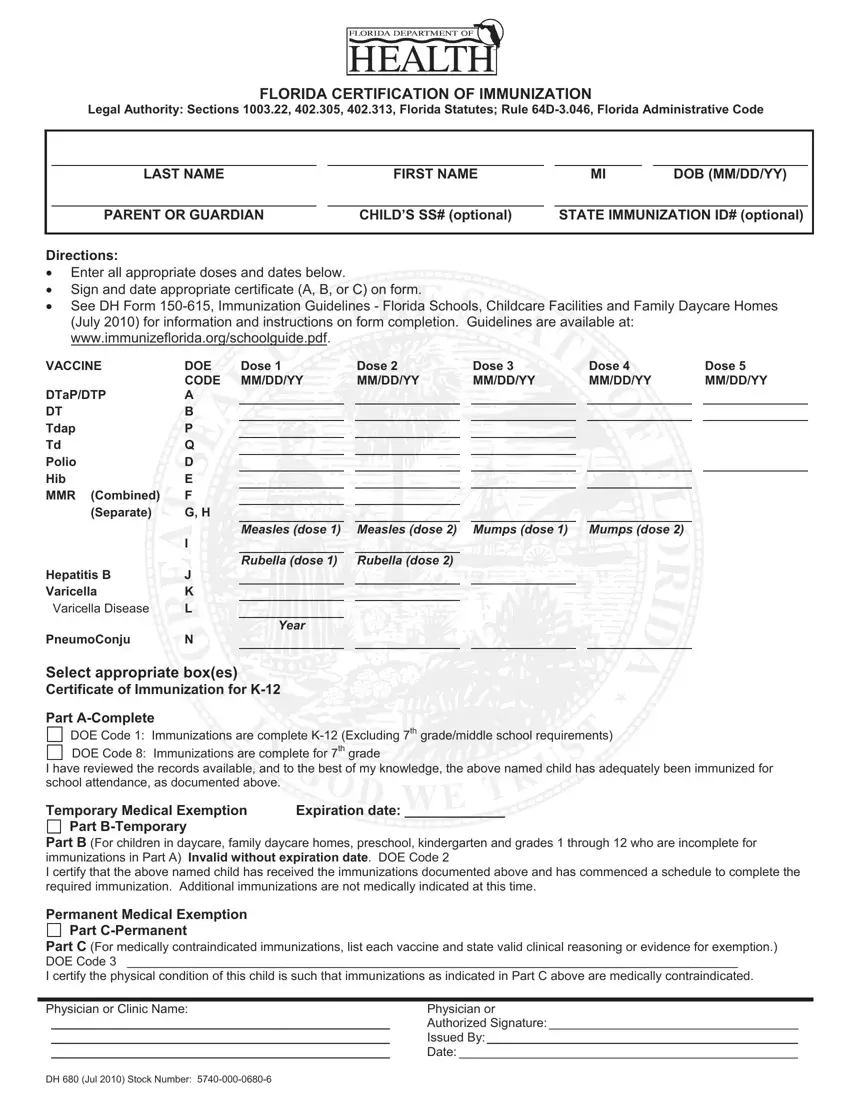
Medical staff start by adding personal details about the child and the child's parent or guardian. That helps connect the record to state tracking systems and prevents mismatches in files, especially when a daycare center enrolled in Florida SHOTS shares immunization updates with public health databases. After that, providers enter vaccination dates across specific rows. Reviewers scan the timeline, checking that required doses appear in the proper order, a quiet yet effective way to prevent overlooked vaccines.
The form also outlines several certification paths:
• Part A confirms full immunization for school or childcare attendance.
• Part B allows temporary attendance while the remaining doses follow a set schedule.
• Part C is specifically for permanent medical exemptions based on valid clinical reasoning, not established religious beliefs or requests made on religious grounds.
Authorized clinic staff sign the chosen section. This form can also be certified with an electronic signature.
Parents often submit the completed record as a document receipt during registration. Schools and childcare facilities may request updates if vaccination schedules change or if new doses appear in medical records.
| Question | Answer |
|---|---|
| Form Name | DH 680 Form |
| Form Length | 1 page |
| Fillable? | Yes |
| Fillable fields | 63 |
| Avg. time to fill out | 15 min |
| Other names | form DH 680 Florida Certification of Immunization, DH 680 form Florida, DH 680 form, Florida immunization PDF |
