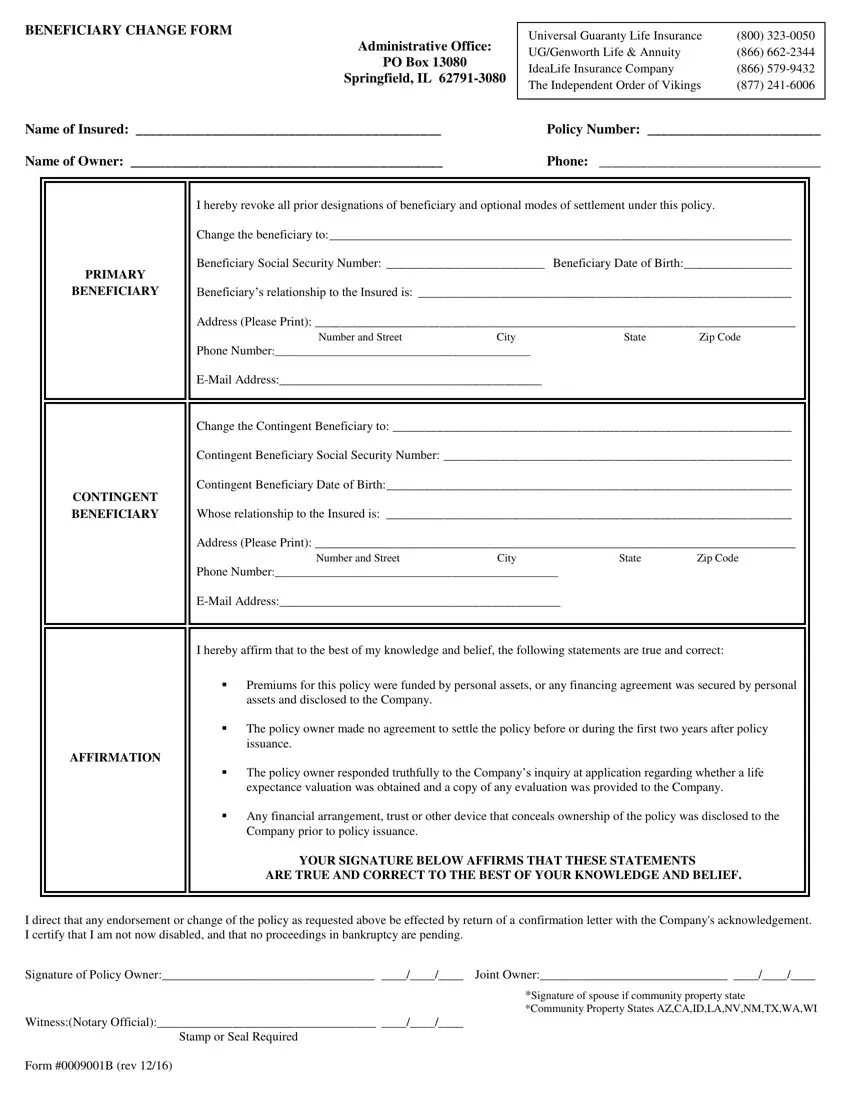
Managing insurance matters efficiently is crucial for policyholders, and the 0009001 form plays a vital role in this process. The primary purpose of this document is to facilitate changes to beneficiaries under a life insurance policy—a significant aspect given the financial security these policies aim to provide to beneficiaries following the policyholder’s demise. The form is used across several insurance providers, including Universal Guaranty Life Insurance, UG/Genworth Life & Annuity, IdeaLife Insurance Company, and The Independent Order of Vikings, demonstrating its wide applicability in the insurance industry. It comprehensively gathers details such as the names of the insured and the policy owner, policy number, and contact information. More importantly, it allows for specifying primary and contingent beneficiaries, requiring pertinent details such as their relationships to the insured, their social security numbers, dates of birth, addresses, and contact information. The form also includes sections for the policy owner to affirm the truthfulness and correctness of information regarding policy funding, any prior agreements on settlement, responses to company inquiries at the application stage, and disclosures about financial arrangements or trusts concealing policy ownership. A space for the policy owner's signature, alongside a witness section typically filled by a notary official, finalizes the request for a beneficiary change, underscoring the formality and legal significance of the procedure. This thorough approach ensures that the policy reflects the current wishes of the policy owner, maintaining the integrity of the policy's intent and providing peace of mind to all parties involved.
| Question | Answer |
|---|---|
| Form Name | Form 0009001 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | primerica beneficiary, primerica multi purpose change form, primerica change of agent form, multi purpose change form primerica |
BENEFICIARY CHANGE FORM
Administrative Office:
PO Box 13080
Springfield, IL
Name of Insured: ____________________________________________
Name of Owner: _____________________________________________
Universal Guaranty Life Insurance |
(800) |
UG/Genworth Life & Annuity |
(866) |
IdeaLife Insurance Company |
(866) |
The Independent Order of Vikings |
(877) |
|
|
Policy Number: _________________________
Phone: ________________________________
PRIMARY
BENEFICIARY
I hereby revoke all prior designations of beneficiary and optional modes of settlement under this policy.
Change the beneficiary to:_________________________________________________________________________
Beneficiary Social Security Number: _________________________ Beneficiary Date of Birth:_________________
Beneficiary’s relationship to the Insured is: ___________________________________________________________
Address (Please Print): _____________________________________________________________________________
Number and StreetCityStateZip Code Phone Number:______________________________________________
CONTINGENT BENEFICIARY
Change the Contingent Beneficiary to: _______________________________________________________________
Contingent Beneficiary Social Security Number: _______________________________________________________
Contingent Beneficiary Date of Birth:________________________________________________________________
Whose relationship to the Insured is: ________________________________________________________________
Address (Please Print): _____________________________________________________________________________
Number and StreetCityStateZip Code Phone Number:___________________________________________________
AFFIRMATION
I hereby affirm that to the best of my knowledge and belief, the following statements are true and correct:
Premiums for this policy were funded by personal assets, or any financing agreement was secured by personal assets and disclosed to the Company.
The policy owner made no agreement to settle the policy before or during the first two years after policy issuance.
The policy owner responded truthfully to the Company’s inquiry at application regarding whether a life expectance valuation was obtained and a copy of any evaluation was provided to the Company.
Any financial arrangement, trust or other device that conceals ownership of the policy was disclosed to the Company prior to policy issuance.
YOUR SIGNATURE BELOW AFFIRMS THAT THESE STATEMENTS
ARE TRUE AND CORRECT TO THE BEST OF YOUR KNOWLEDGE AND BELIEF.
I direct that any endorsement or change of the policy as requested above be effected by return of a confirmation letter with the Company's acknowledgement. I certify that I am not now disabled, and that no proceedings in bankruptcy are pending.
Signature of Policy Owner:__________________________________ ____/____/____ Joint Owner:______________________________ ____/____/____
*Signature of spouse if community property state
*Community Property States AZ,CA,ID,LA,NV,NM,TX,WA,WI
Witness:(Notary Official):___________________________________ ____/____/____
Stamp or Seal Required
Form #0009001B (rev 12/16)
