
form duty online can be completed online with ease. Just make use of FormsPal PDF tool to complete the job in a timely fashion. Our tool is constantly evolving to deliver the best user experience possible, and that's because of our resolve for constant improvement and listening closely to testimonials. Here's what you'd have to do to get going:
Step 1: Press the "Get Form" button above. It will open up our pdf editor so you could begin completing your form.
Step 2: Once you access the PDF editor, you will notice the document prepared to be completed. Other than filling in different blanks, you may as well perform various other actions with the form, specifically adding your own text, modifying the initial text, inserting images, affixing your signature to the PDF, and a lot more.
If you want to fill out this PDF document, ensure you enter the information you need in every single blank:
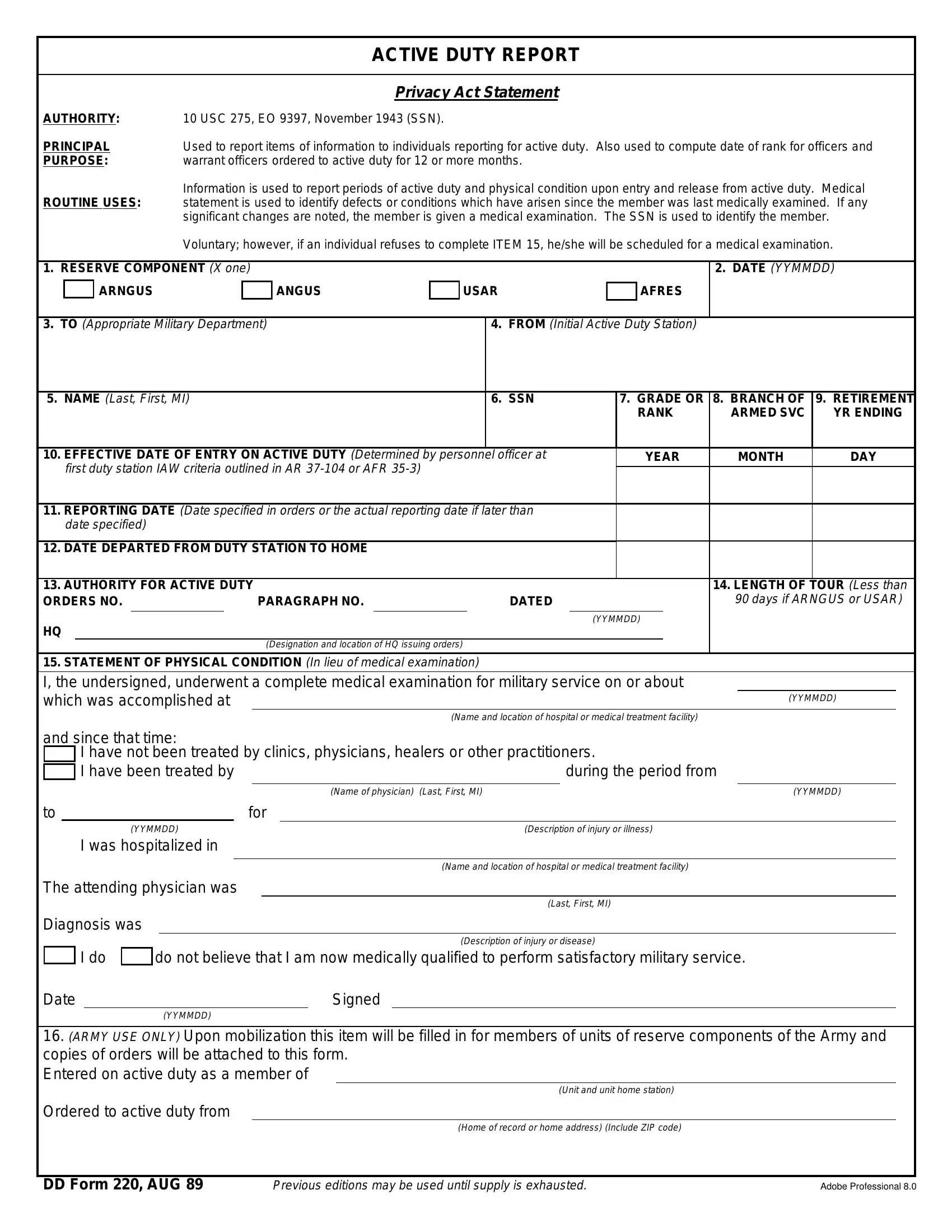
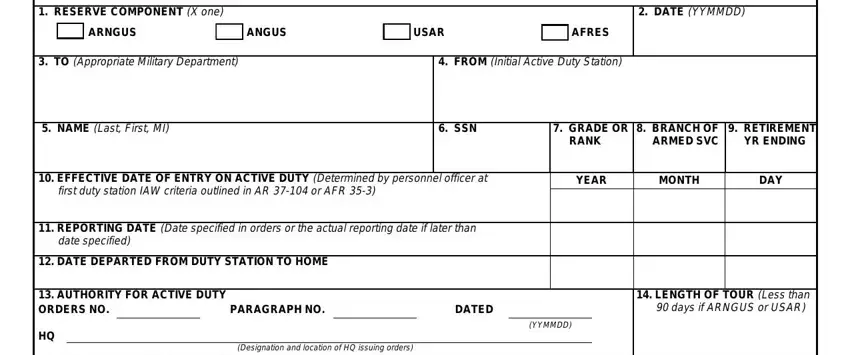
1. You have to fill out the form duty online correctly, thus be careful when working with the sections that contain these specific blank fields:
2. Your next part is usually to submit these particular fields: STATEMENT OF PHYSICAL CONDITION, Nameand location ofhospital or, YYMMDD, and since that time, I have not been treated by clinics, during the period from, Name ofphysician Last First MI, YYMMDD, for, YYMMDD, I was hospitalized in, The attending physician was, Diagnosis was, Descriptionof injury or illness, and Nameand location ofhospital or.
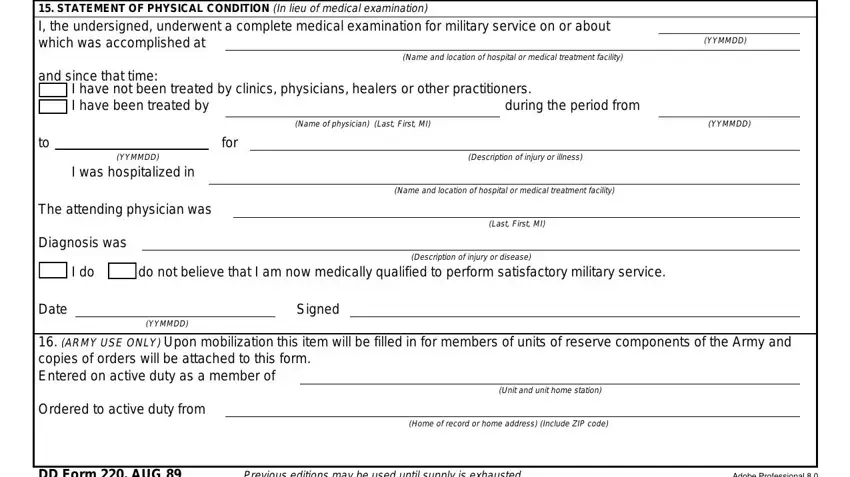
It is possible to get it wrong while filling in your Nameand location ofhospital or, so ensure that you go through it again before you send it in.
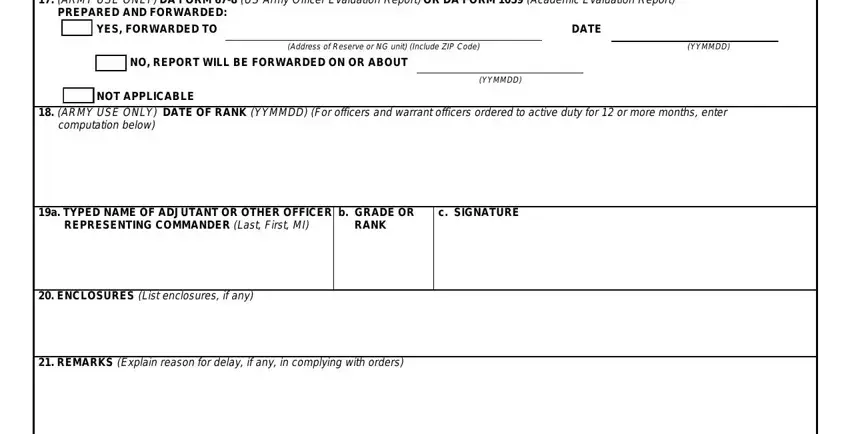
3. Completing ARMY USE ONLYDA FORM USArmy, PREPARED AND FORWARDED, YES FORWARDED TO, DATE, Address ofReserve orNGunit Include, YYMMDD, NO REPORT WILL BE FORWARDED ON OR, YYMMDD, NOT APPLICABLE, ARMY USE ONLY DATE OF RANK, computation below, a TYPED NAME OF ADJUTANT OR OTHER, REPRESENTING COMMANDER Last FirstMI, b GRADE OR, and RANK is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Prior to getting to the next stage, check that all form fields are filled in properly. The moment you are satisfied with it, click “Done." Join us today and immediately get form duty online, set for downloading. All modifications you make are saved , which enables you to customize the document later on as required. FormsPal is focused on the privacy of all our users; we make sure all personal data going through our system is confidential.