
You'll be able to complete form chronic disease instantly with the help of our online PDF editor. The editor is consistently improved by our staff, getting awesome functions and growing to be much more versatile. Here is what you'll have to do to get going:
Step 1: Access the PDF doc in our editor by clicking on the "Get Form Button" in the top part of this page.
Step 2: This tool allows you to change nearly all PDF documents in a range of ways. Change it by including any text, correct what is already in the PDF, and add a signature - all within the reach of a few mouse clicks!
This PDF form needs some specific information; in order to guarantee accuracy, make sure you take heed of the recommendations further on:
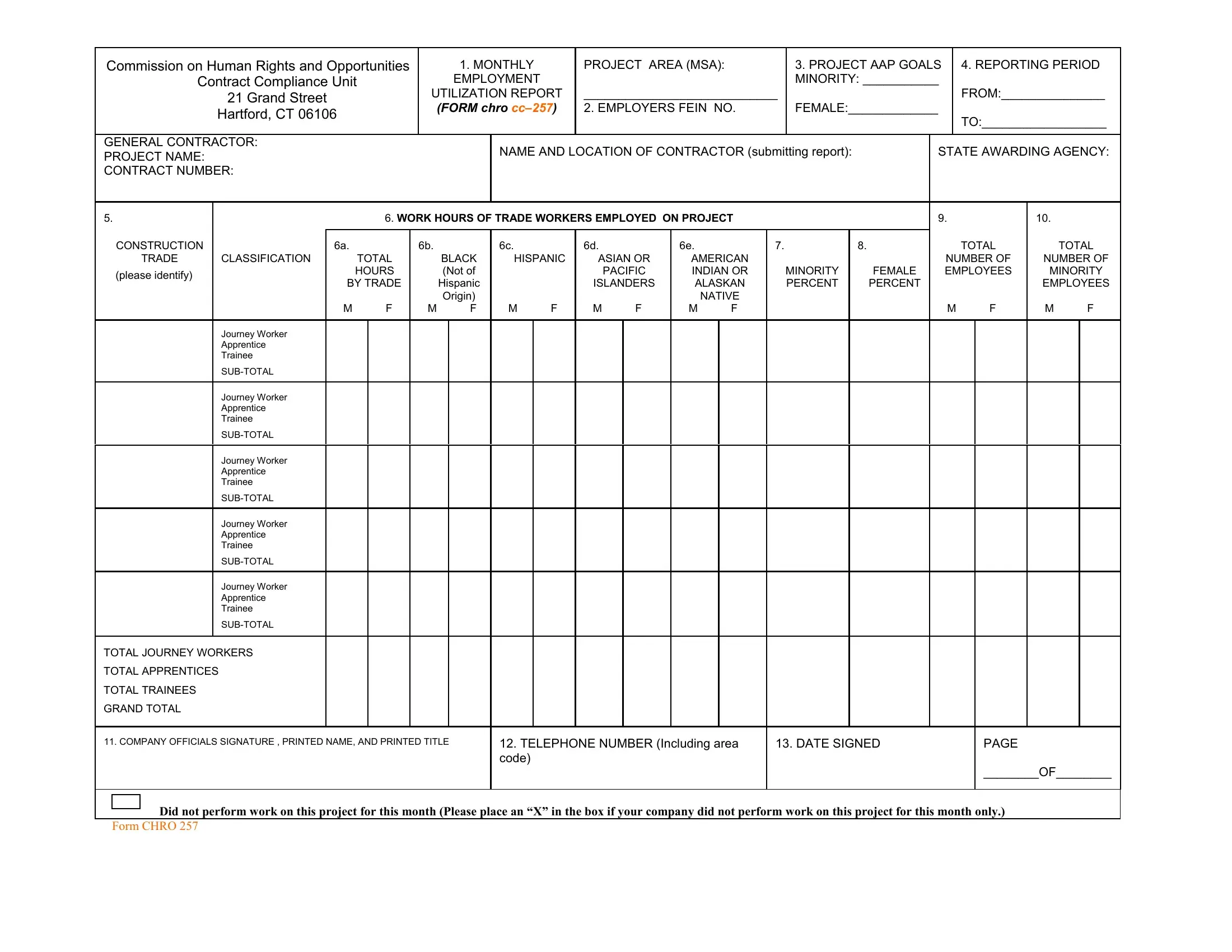
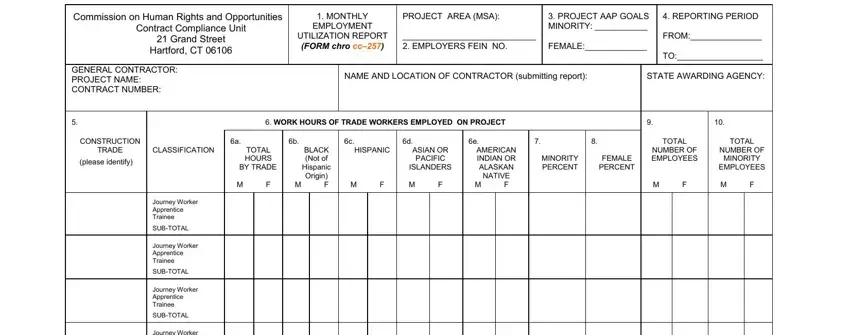
1. Before anything else, while filling out the form chronic disease, start with the section containing next blanks:
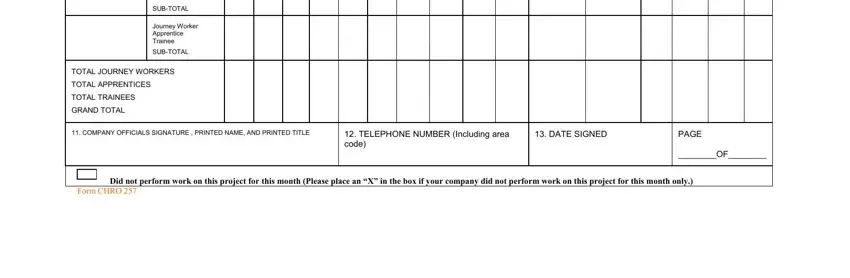
2. Once the previous segment is complete, you have to add the essential details in Journey Worker Apprentice Trainee, SUBTOTAL, Journey Worker Apprentice Trainee, SUBTOTAL, TOTAL JOURNEY WORKERS, TOTAL APPRENTICES, TOTAL TRAINEES, GRAND TOTAL, COMPANY OFFICIALS SIGNATURE, TELEPHONE NUMBER Including area, DATE SIGNED, PAGE OF, Did not perform work on this, and Form CHRO allowing you to move forward further.
3. Completing Commission on Human Rights and, Contract Compliance Unit, Grand Street, Hartford CT, MONTHLY, EMPLOYMENT, UTILIZATION REPORT FORM chro ccA, PROJECT AREA MSA EMPLOYERcid FEIN, PROJECT AAP GOALS MINORITY FEMALE, REPORTING PERIOD FROM TO, NAME AND LOCATION OF CONTRACTOR, STATE AWARDING AGENCY, GENERAL CONTRACTOR PROJECT NAME, WORK HOURS OF WORKERS OTHER THAN, and ON SITE PERSONNEL OTHER THAN TRADE is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
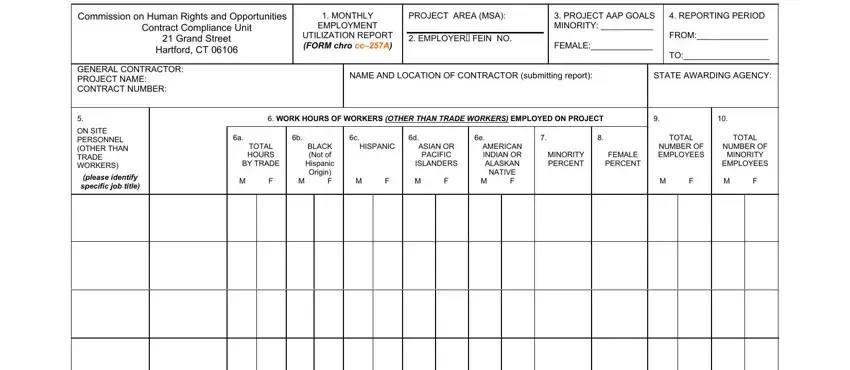
Concerning MONTHLY and ON SITE PERSONNEL OTHER THAN TRADE, make certain you review things in this section. These two are the most significant fields in the PDF.
4. You're ready to fill in this fourth segment! Here you have these GRAND TOTAL WORKERS, COMPANY OFFICIALS SIGNATURE, TELEPHONE NUMBER Including area, DATE SIGNED, PAGE OF, Did not perform work on this, and Form CHRO a form blanks to complete.
Step 3: Prior to finalizing the form, make certain that blank fields were filled in right. As soon as you’re satisfied with it, click on “Done." Right after creating afree trial account at FormsPal, you'll be able to download form chronic disease or email it at once. The form will also be readily available from your personal account menu with your every change. FormsPal ensures your information privacy by having a protected method that never saves or shares any kind of private information involved in the process. Feel safe knowing your documents are kept protected each time you work with our service!