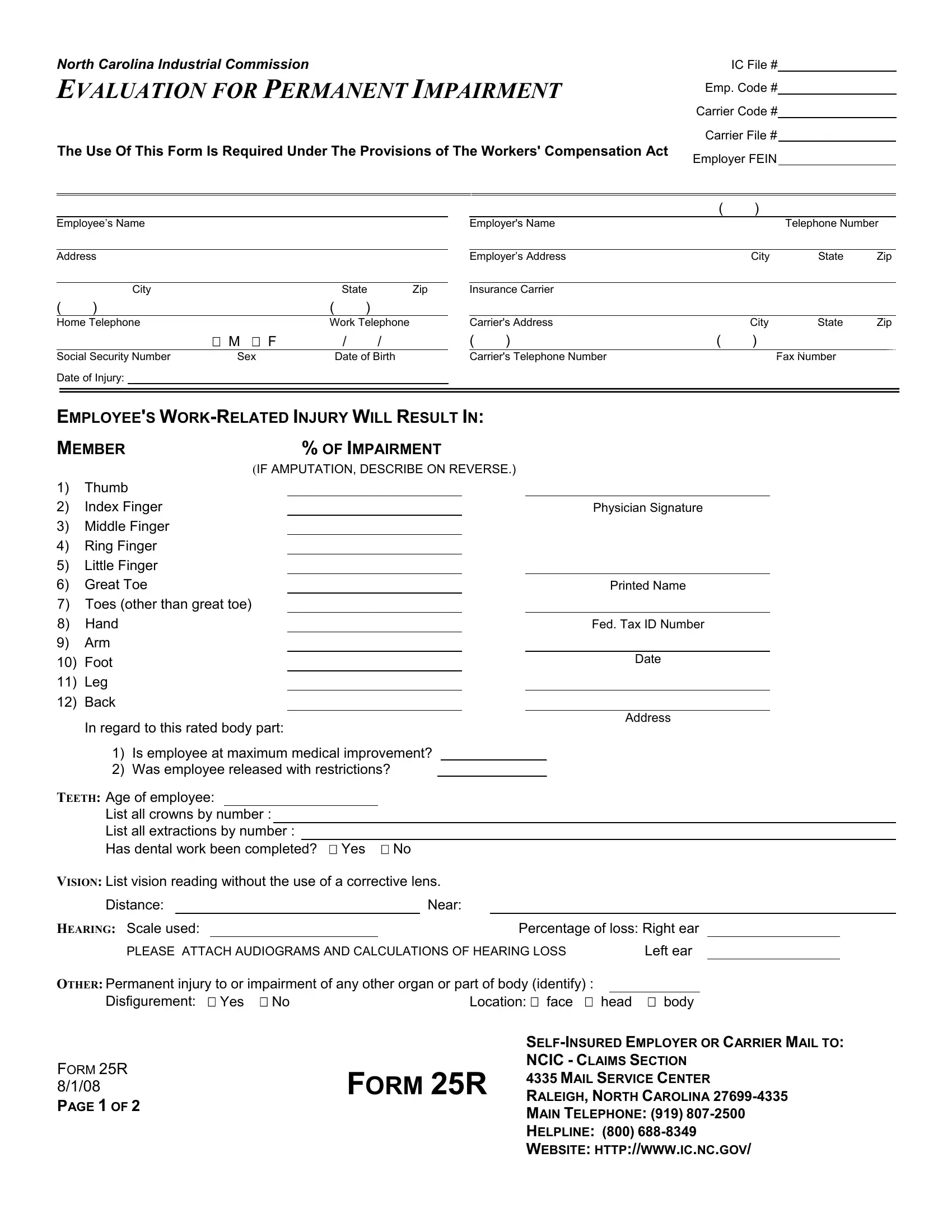
In the realm of workers' compensation, the 25R Form emerges as a pivotal document mandated by the provisions of the Workers' Compensation Act, specifically within the jurisdiction of North Carolina. This form is meticulously designed to evaluate the extent of an employee's permanent impairment resulting from a work-related injury. It encompasses a comprehensive assessment ranging from the designated body parts such as thumbs, fingers, and back, to other areas including dental, vision, and hearing impairments. The process it outlines intends not just to document the percentage of impairment experienced by the employee but also to determine whether the employee has reached maximum medical improvement and if they have been released with restrictions. The form necessitates the detailed input of the evaluating physician, alongside vital employee information such as social security number, address, and the specific details of the injury sustained. Moreover, it stipulates guidelines for computing compensation for amputations, thereby providing a structured approach to quantifying compensation benefits. The requirement for this form underscores the legal framework aimed at ensuring fair compensation for employees who have suffered work-related injuries, promoting a gesture of accountability from employers and insurance carriers. Detailed instructions for the submission of the completed form highlight the formal process involved, ensuring both the employee and their attorney (if applicable) receive a copy, with the original being directed to the Industrial Commission.
| Question | Answer |
|---|---|
| Form Name | Form 25R |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 25r form, 25 r, 25 r form, form 25r pdf north carolina |