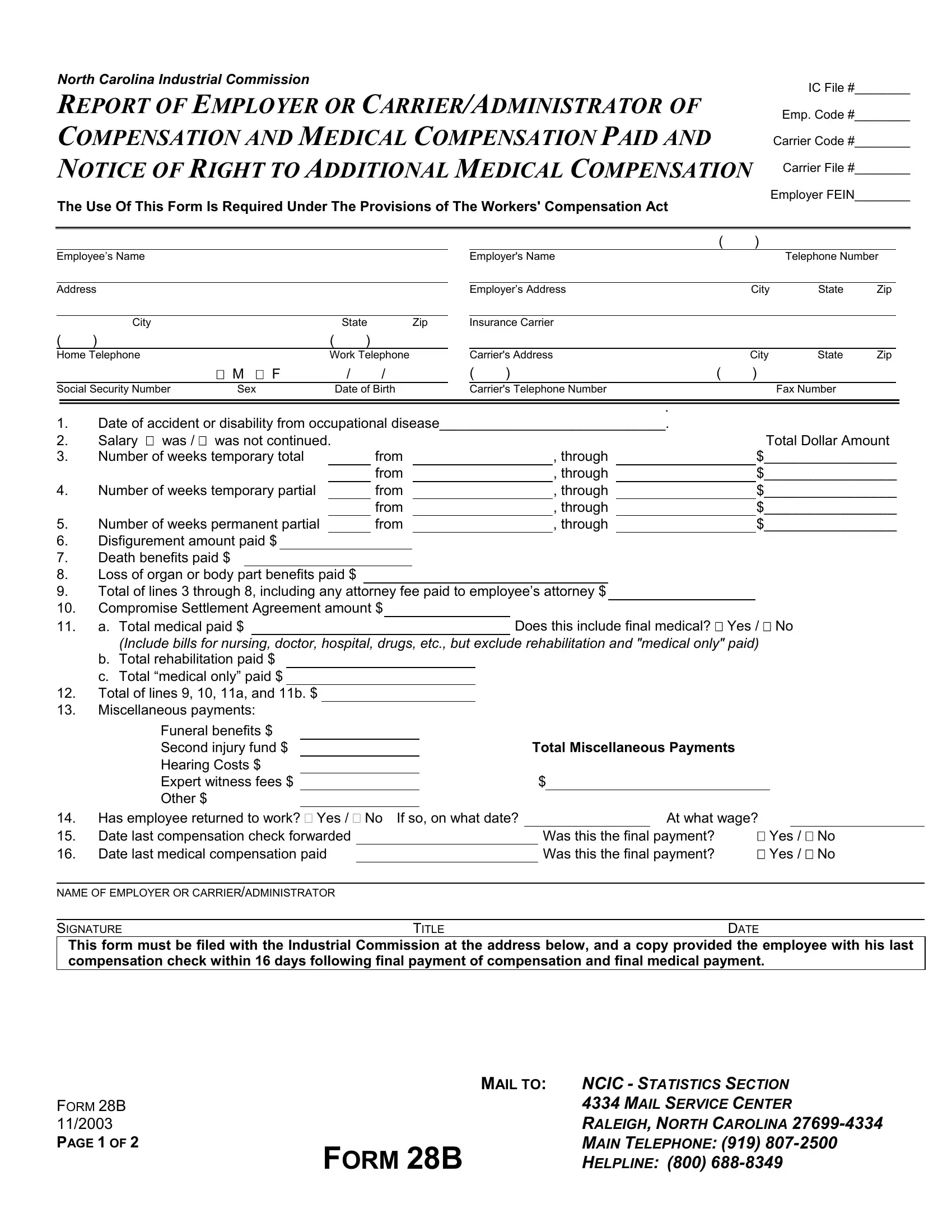
Under the framework of the Workers' Compensation Act, Form 28B plays a crucial role in the administration of compensation and medical benefits to employees who find themselves injured or disabled as a result of their employment. It is a comprehensive document that not only captures the essence of the compensation paid but also marks the closure of such payments. Employed by employers or carrier/administrators, this form reports the details of compensation and medical benefits disbursed to the affected employee. It includes sections for reporting temporary total, temporary partial, and permanent partial payments, in addition to detailing disfigurement, death benefits, and loss of organ benefits paid out. One of its key features is the mandate to report the finality of medical payments and any notifications regarding the right to additional medical compensation, making it an essential document for both the processing of workers' compensation claims and ensuring the rights of employees for future medical assistance. The form requires meticulous input of data ranging from the accident's details, compensation specifics, to the information on the final payment. The obligation to file this form with the North Carolina Industrial Commission and provide a copy to the employee within a stipulated time period underscores its importance in the regulatory landscape of workers' compensation, emphasizing transparency, accountability, and the ongoing right to medical care.
| Question | Answer |
|---|---|
| Form Name | Form 28B |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 1994, ncic form 28b, fillable, North_Carolina |
NORTH CAROLINA INDUSTRIAL COMMISSION
IC File #________
REPORT OF EMPLOYER OR CARRIER/ADMINISTRATOR OF |
Emp. Code #________ |
|
|
COMPENSATION AND MEDICAL COMPENSATION PAID AND |
Carrier Code #________ |
NOTICE OF RIGHT TO ADDITIONAL MEDICAL COMPENSATION |
Carrier File #________ |
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act |
Employer FEIN________ |
|
Employee’s Name
Address
|
City |
|
|
State |
Zip |
( |
) |
|
( |
) |
|
Home Telephone |
|
Work Telephone |
|||
|
|
M F |
|
/ |
/ |
Social Security Number |
Sex |
|
Date of Birth |
||
|
|
( |
) |
|
|
Employer's Name |
|
|
Telephone Number |
||
|
|
|
|
|
|
Employer’s Address |
|
City |
State |
Zip |
|
|
|
|
|
|
|
Insurance Carrier |
|
|
|
|
|
|
|
|
|
|
|
Carrier's Address |
|
City |
State |
Zip |
|
( |
) |
( |
) |
|
|
Carrier's Telephone Number
.
1.Date of accident or disability from occupational disease_____________________________.
2. |
Salary was / was not continued. |
|
|
|
|
Total Dollar Amount |
|
3. |
Number of weeks temporary total |
|
from |
|
, through |
|
$_________________ |
|
|
|
from |
|
, through |
|
$_________________ |
4. |
Number of weeks temporary partial |
|
from |
|
, through |
|
$_________________ |
|
|
|
from |
|
, through |
|
$_________________ |
5. |
Number of weeks permanent partial |
from |
|
, through |
$_________________ |
||
6.Disfigurement amount paid $
7.Death benefits paid $
8.Loss of organ or body part benefits paid $
9.Total of lines 3 through 8, including any attorney fee paid to employee’s attorney $
10.Compromise Settlement Agreement amount $
11. |
a. Total medical paid $ |
|
|
Does this include final medical? Yes / No |
|
(Include bills for nursing, doctor, hospital, drugs, etc., but exclude rehabilitation and "medical only" paid) |
|||
b.Total rehabilitation paid $
c.Total “medical only” paid $
12.Total of lines 9, 10, 11a, and 11b. $
13.Miscellaneous payments:
Funeral benefits $ Second injury fund $ Hearing Costs $ Expert witness fees $ Other $
14. Has employee returned to work? Yes / No If so, on what date?
15. Date last compensation check forwarded
16. Date last medical compensation paid
NAME OF EMPLOYER OR CARRIER/ADMINISTRATOR
SIGNATURE |
TITLE |
DATE |
This form must be filed with the Industrial Commission at the address below, and a copy provided the employee with his last compensation check within 16 days following final payment of compensation and final medical payment.
FORM 28B 11/2003
PAGE 1 OF 2
|
MAIL TO: NCIC - STATISTICS SECTION |
|
4334 MAIL SERVICE CENTER |
|
RALEIGH, NORTH CAROLINA |
FORM 28B |
MAIN TELEPHONE: (919) |
HELPLINE: (800) |
FOR INDUSTRIAL COMMISSION USE ONLY
Days |
____________________ |
Compensation Paid |
$____________________ |
Medical |
$____________________ |
IC Code: |
____________________ |
IMPORTANT NOTICE TO EMPLOYEE CLAIMING
ADDITIONAL WEEKLY COMPENSATION CHECKS
OR LUMP SUM PAYMENT
If you claim further compensation, you must notify the Industrial Commission in writing within two years from the date of receipt of your last compensation check or your rights to these benefits may be lost.
IMPORTANT NOTICE TO EMPLOYEE
CLAIMING ADDITIONAL MEDICAL BENEFITS
INJURED BEFORE JULY 5, 1994
If your injury occurred before July 5, 1994, you are entitled to medical compensation as long as it is reasonably necessary, related to your workers' compensation case, and authorized by the carrier or the Industrial Commission.
IMPORTANT NOTICE TO EMPLOYEE
CLAIMING ADDITIONAL MEDICAL BENEFITS
INJURED ON OR AFTER JULY 5, 1994
If your injury occurred on or after July 5, 1994, your right to future medical compensation will depend on several factors. Your right to payment of future medical compensation will terminate two years after your employer or carrier/administrator last pays any medical compensation or other compensation, whichever occurs last. If you think you will need future medical compensation, you must apply to the Industrial Commission in writing within two years, or your right to these benefits may be lost. To apply you may also use Industrial Commission Form 18M.
DEFINITION OF MEDICAL COMPENSATION
The term "medical compensation" means medical, surgical, hospital, nursing and rehabilitative services, and medicines, sick travel, and other treatment, including medical and surgical supplies, as may reasonably be required to effect a cure or give relief, and for such additional time, as in the judgment of the Industrial Commission, will tend to lessen the period of disability; and any original artificial members as may reasonably be necessary at the end of the healing period, and the replacement of such artificial members when reasonably necessitated by ordinary use or medical circumstances. N.C. Gen. Stat. §
NEED ASSISTANCE?
If you have questions or need help and you do not have an attorney, you may contact the Industrial Commission’ Ombudsman at
(800)
FORM 28B 11/2003
PAGE 2 OF 2
|
MAIL TO: NCIC - STATISTICS SECTION |
|
4334 MAIL SERVICE CENTER |
|
RALEIGH, NORTH CAROLINA |
FORM 28B |
MAIN TELEPHONE: (919) |
HELPLINE: (800) |