
Handling PDF forms online is actually very easy with our PDF editor. Anyone can fill out hhsc form 3613 here and use several other functions we provide. The editor is constantly maintained by us, receiving useful features and growing to be much more convenient. Getting underway is simple! Everything you need to do is follow these basic steps down below:
Step 1: First, access the pdf editor by pressing the "Get Form Button" at the top of this webpage.
Step 2: The editor offers you the capability to customize your PDF form in many different ways. Improve it with any text, correct original content, and include a signature - all at your convenience!
Completing this PDF calls for attention to detail. Make sure that all mandatory blanks are filled in correctly.
1. Fill out your hhsc form 3613 with a selection of necessary blank fields. Note all of the important information and ensure there is nothing left out!
2. The third part is usually to fill out the next few blanks: City State ZIP Code, County, Area Code and Telephone No, Fax Area Code and Telephone No, Parent, BranchAlternate Delivery Site, Confidential Document, This communication including any, For Home and Community Support, Home Health Personal Assistance, and Form.
3. Through this step, examine DADS Intake ID No, Date Reported to DADS, Time Reported, DFPS Call ID No, License No, Area Code and Telephone No, Fax Area Code and Telephone No, City, ZIP Code, Who made the allegation, County, When, Provider Type, HCSSA, and Name. All these need to be filled in with highest accuracy.
4. This next section requires some additional information. Ensure you complete all the necessary fields - If applicable describe any special, Age at the time of the allegation, Services Provided type number of, Independently ambulatory, Yes, No Interviewable, Yes, No Capacity to make informed, Yes, Known history of, Combativeness, Sexual misconduct, Yes Yes, No No, and Similar allegations - to proceed further in your process!
5. To finish your document, the particular area includes a few extra blanks. Filling in DADS Intake ID No, Agency Name, License No, How was the AP identified, By Name, By Description, Other, The AP, Denied, Confirmed, History of similar allegations, Yes, Did investigation reveal the, Statement attached signed and, and Yes should finalize everything and you can be done in no time!
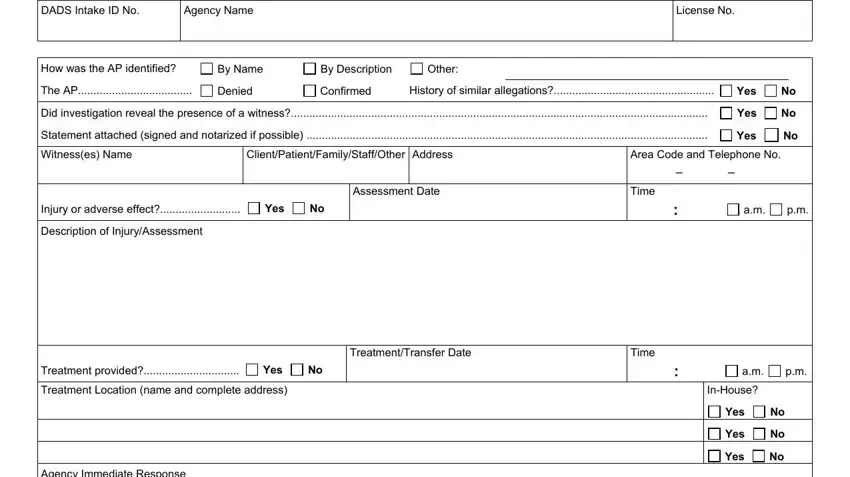
In terms of Yes and License No, be certain that you do everything right here. Both these are the key fields in the file.
Step 3: Before moving forward, check that all blanks have been filled out the correct way. As soon as you determine that it's correct, press “Done." Sign up with us right now and immediately access hhsc form 3613, set for download. All changes made by you are saved , meaning you can modify the pdf at a later point if necessary. FormsPal guarantees safe form completion devoid of personal data recording or distributing. Rest assured that your details are secure with us!