
Making use of the online PDF editor by FormsPal, you may fill out or alter hhsc ipc form right here and now. To have our tool on the leading edge of efficiency, we aim to put into practice user-driven capabilities and enhancements regularly. We're at all times happy to receive feedback - help us with remolding PDF editing. Here's what you'd have to do to begin:
Step 1: Access the form inside our editor by pressing the "Get Form Button" in the top area of this page.
Step 2: The editor grants the opportunity to work with PDF files in a variety of ways. Change it by including customized text, correct original content, and add a signature - all at your fingertips!
Filling out this document demands attentiveness. Make sure every single field is done accurately.
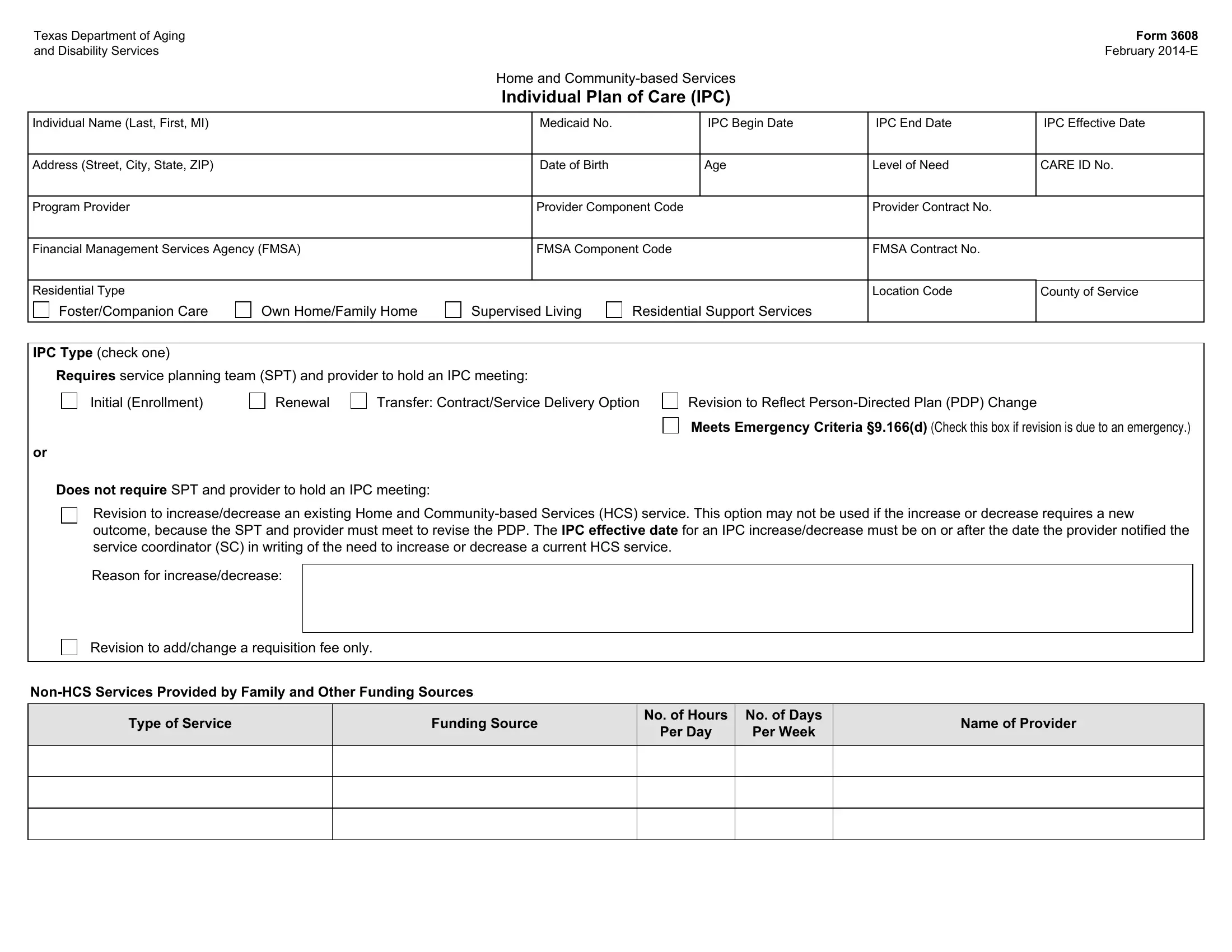
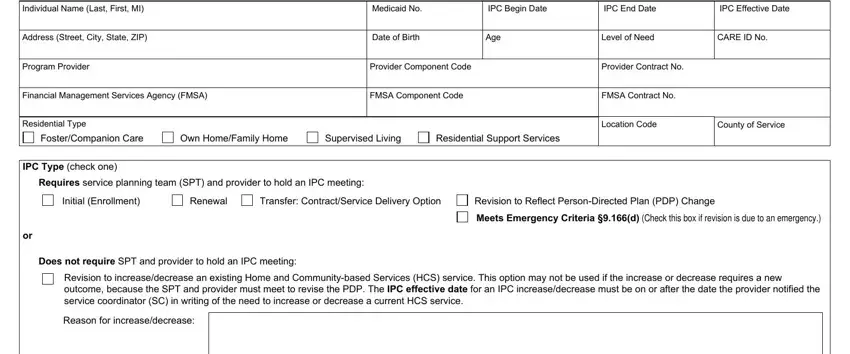
1. Start filling out your hhsc ipc form with a group of essential blank fields. Consider all of the information you need and make sure absolutely nothing is neglected!
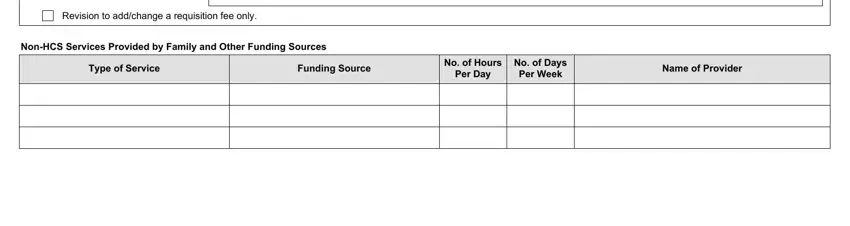
2. When the previous section is completed, go on to enter the applicable details in these - Revision to addchange a, NonHCS Services Provided by Family, Type of Service, Funding Source, No of Hours, No of Days, Per Day, Per Week, and Name of Provider.
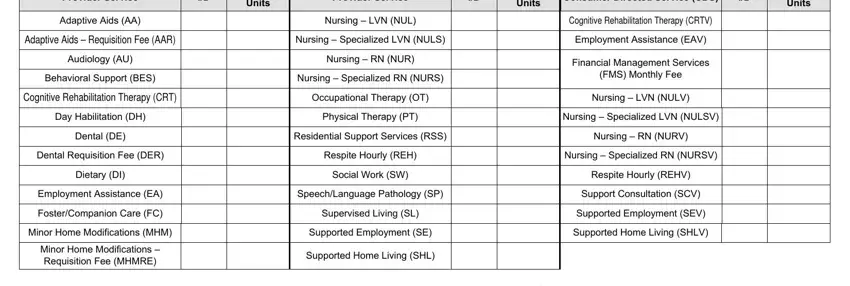
3. This next step is generally hassle-free - fill out every one of the blanks in Provider Service, Units, Provider Service, Units, Consumer Directed Service CDS, Units, Adaptive Aids AA, Nursing LVN NUL, Cognitive Rehabilitation Therapy, Adaptive Aids Requisition Fee AAR, Nursing Specialized LVN NULS, Employment Assistance EAV, Audiology AU, Nursing RN NUR, and Behavioral Support BES in order to finish this segment.
4. To go forward, this next step will require completing a few empty form fields. Examples of these are Totals from CARE Screen C for all, CDS Estimated Annual Total, Program Provider Estimated Annual, IPC Estimated Annual Total, Are any services staffed by a, and Yes, which are essential to carrying on with this particular form.
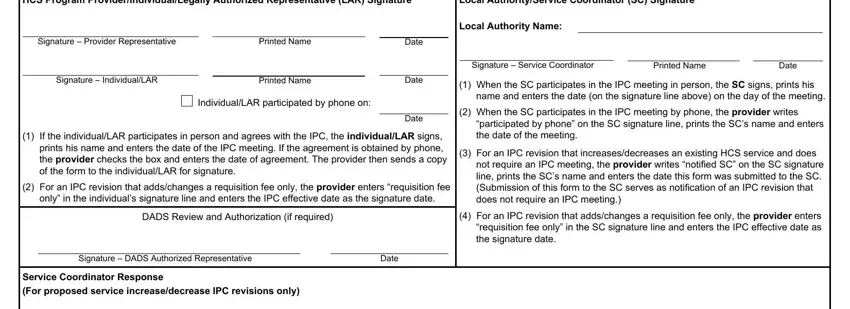
5. The form needs to be wrapped up by dealing with this area. Here you'll see a comprehensive list of form fields that need accurate details for your form usage to be accomplished: HCS Program, Local AuthorityService Coordinator, Signature Provider Representative, Printed Name, Signature IndividualLAR, Printed Name, IndividualLAR participated by, Date, Date, Date, If the individualLAR participates, For an IPC revision that, only in the individuals signature, DADS Review and Authorization if, and Signature DADS Authorized.
People who use this document generally get some things incorrect while completing Date in this area. You need to go over everything you enter right here.
Step 3: Revise the details you have inserted in the blank fields and hit the "Done" button. Join us today and instantly get hhsc ipc form, available for download. Each edit made is handily kept , meaning you can modify the form at a later stage if necessary. We don't share or sell the information you type in while completing documents at our website.