
In case you need to fill out adult family license, you don't have to download any kind of applications - simply try our PDF tool. Our expert team is relentlessly endeavoring to expand the tool and help it become much faster for clients with its many features. Discover an endlessly revolutionary experience now - check out and uncover new opportunities as you go! It merely requires a few basic steps:
Step 1: Click on the "Get Form" button above on this page to get into our tool.
Step 2: With the help of our state-of-the-art PDF editor, it is possible to accomplish more than merely fill out blanks. Edit away and make your documents appear faultless with custom textual content added, or fine-tune the file's original content to perfection - all that accompanied by the capability to incorporate stunning graphics and sign the file off.
Completing this form calls for focus on details. Make sure that all mandatory fields are filled out properly.
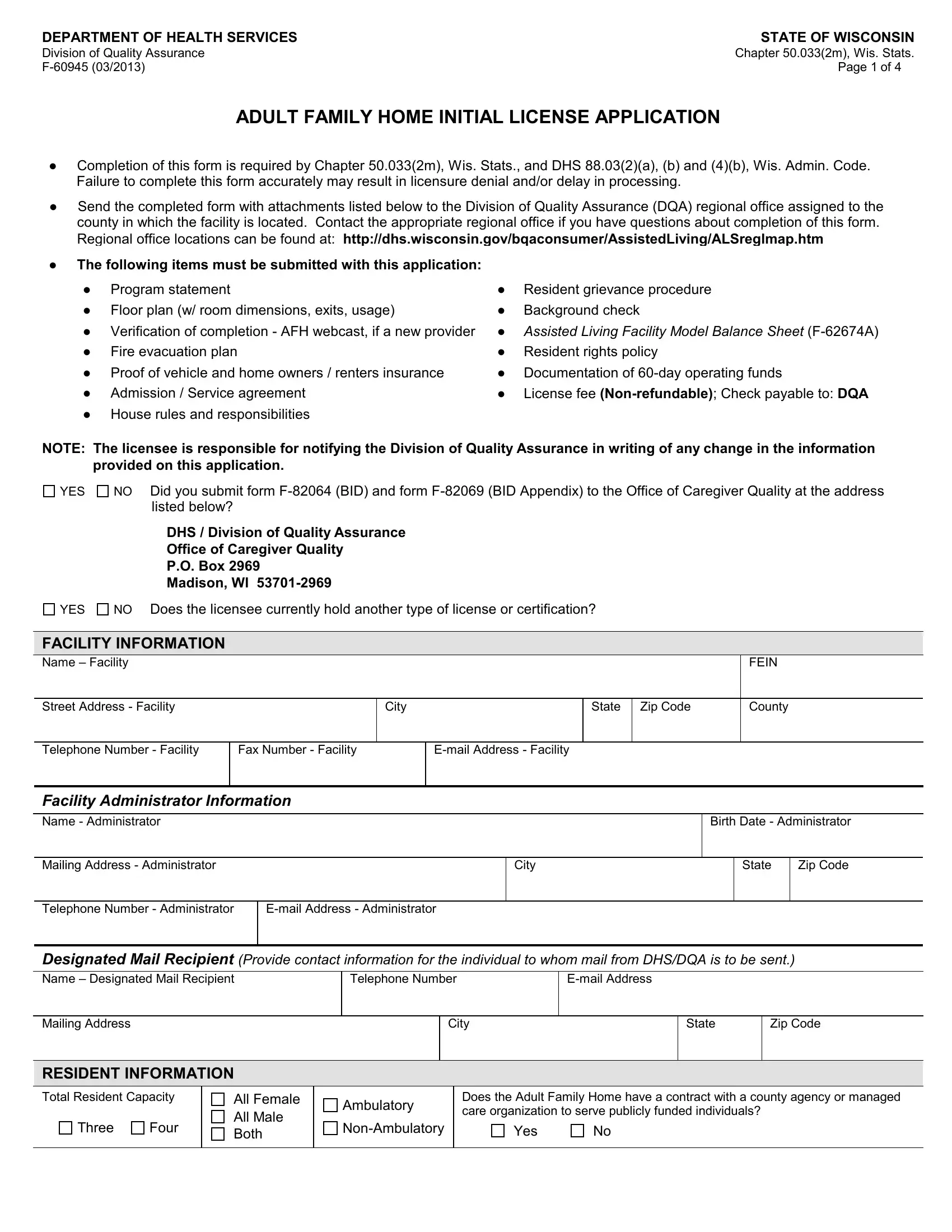
1. The adult family license usually requires specific details to be typed in. Ensure that the following fields are completed:
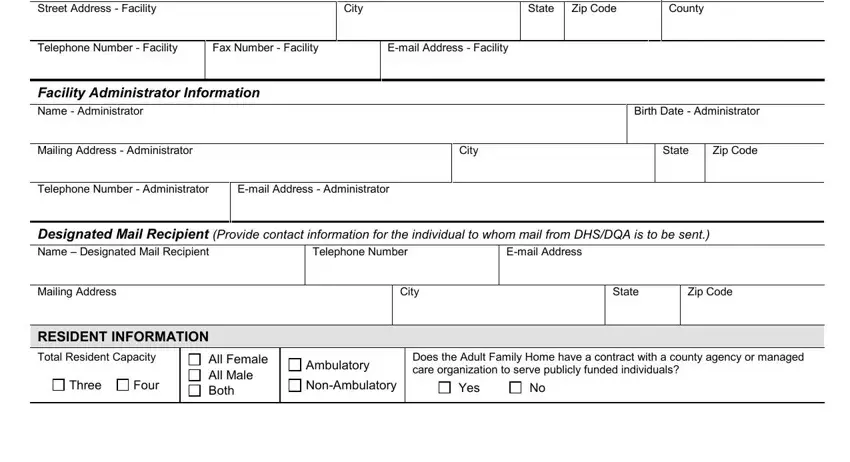
2. When this part is completed, proceed to type in the relevant details in these: Street Address Facility, City, State, Zip Code, County, Telephone Number Facility, Fax Number Facility, Email Address Facility, Facility Administrator Information, Mailing Address Administrator, Telephone Number Administrator, Email Address Administrator, City, Birth Date Administrator, and State.
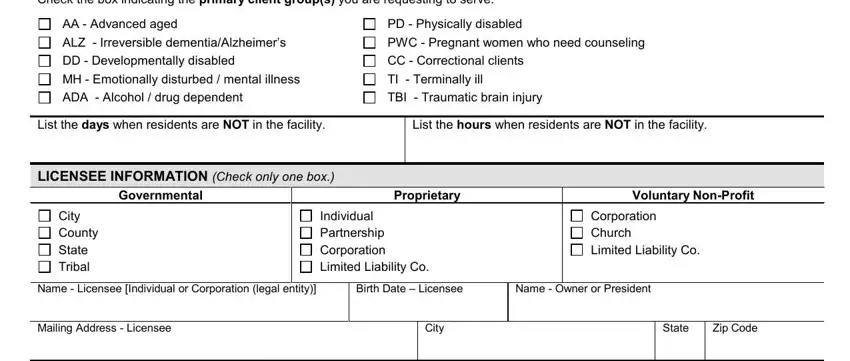
3. In this specific step, review Check the box indicating the, AA Advanced aged ALZ, PD Physically disabled PWC, List the days when residents are, LICENSEE INFORMATION Check only, List the hours when residents are, Governmental, Proprietary, Voluntary NonProfit, City County State Tribal, Individual Partnership Corporation, Corporation Church Limited, Name Licensee Individual or, Birth Date Licensee, and Name Owner or President. Each of these need to be filled out with highest precision.
4. Your next section needs your attention in the subsequent places: Telephone Number Licensee, Email Address Licensee, If the licensee currently holds, License Type, Certification Type, Registration Type, Foster Home children Group Foster, Youth, Alcohol and Other Drug Abuse, Residential Care Apartment, Complex, Complex, Other Specify, Shelter Care children Adult Family, and FIT AND QUALIFIED. It is important to fill in all required information to go onward.
Many people generally make errors when filling out License Type in this area. You should review what you type in right here.
5. This pdf should be wrapped up within this segment. Below you'll find a full list of blank fields that need accurate information to allow your form usage to be accomplished: Was the facility program, No If yes provide the name address, Yes, Has the licensee ever had a, not renewed Yes, and No If yes specify the type of.
Step 3: Right after you've reread the details you given, simply click "Done" to complete your FormsPal process. Download your adult family license when you subscribe to a 7-day free trial. Immediately gain access to the form in your FormsPal account, along with any edits and changes being automatically kept! FormsPal provides risk-free document editor devoid of personal data recording or sharing. Feel comfortable knowing that your details are safe here!