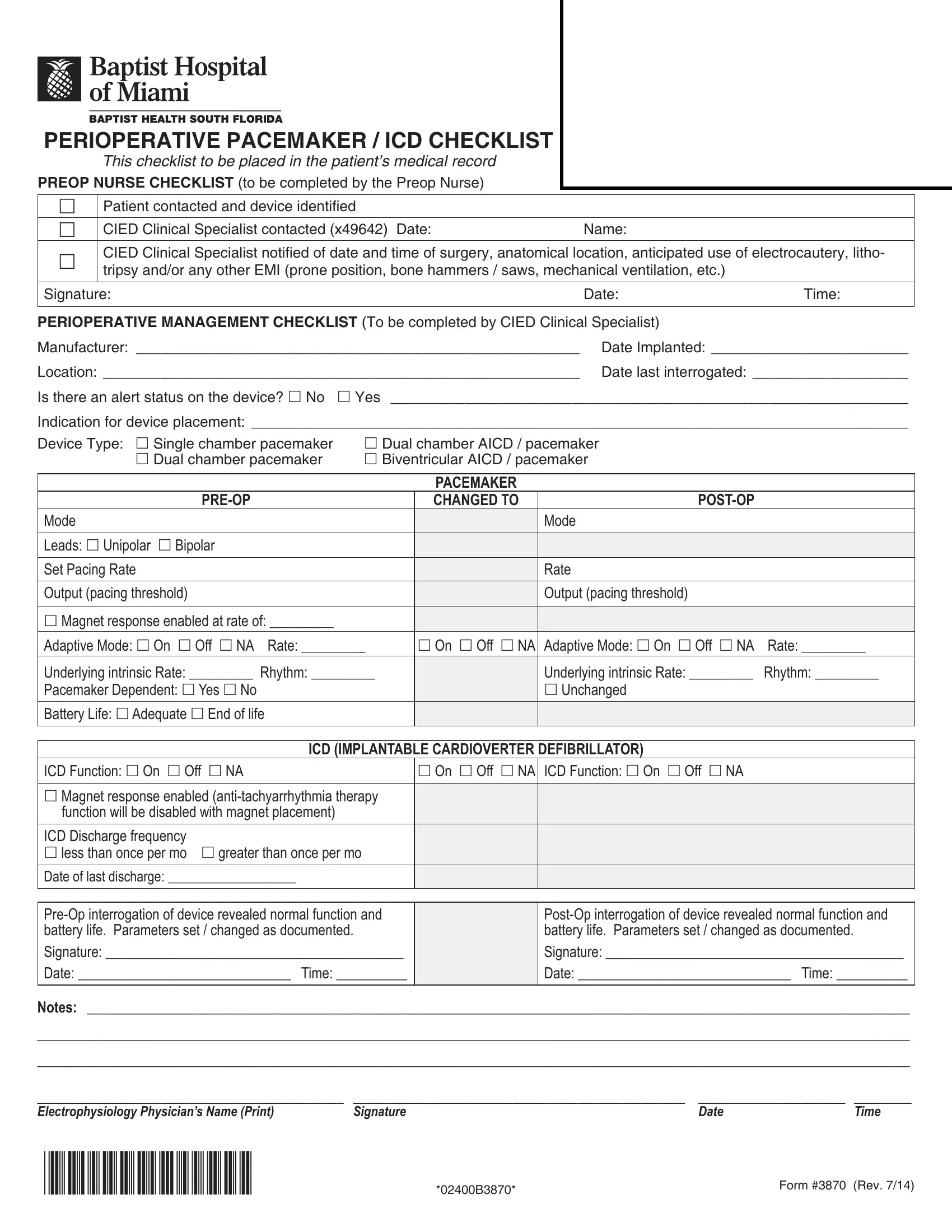
In the complex and highly specialized world of healthcare, specific procedures and protocols are put in place to ensure patient safety and successful outcomes, particularly when it involves individuals with implanted medical devices such as pacemakers or implantable cardioverter-defibrillators (ICDs). The 3870 form, known as the Perioperative Pacemaker/ICD Checklist, stands as a critical tool within this framework, designed to guide healthcare professionals through the necessary steps to prepare and manage patients with these devices during surgical procedures. This meticulously detailed checklist is divided into two main sections: the Preop Nurse Checklist and the Perioperative Management Checklist, to be completed by the CIED Clinical Specialist. It covers a comprehensive range of considerations from verifying the patient and device information, assessing the device's function and battery life, to adjusting settings to accommodate the surgical environment and potential electromagnetic interference. The ultimate goals of using form 3870 are to maintain the functionality of the cardiac device, ensure patient safety, and mitigate any risks associated with surgery. This document is placed in the patient's medical record and serves as an essential communication tool among the medical team members, highlighting the importance of detailed preparation and post-operative care for patients with these life-sustaining devices.
| Question | Answer |
|---|---|
| Form Name | Form 3870 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CIED, form 3870, irs form 3870, EMI |
