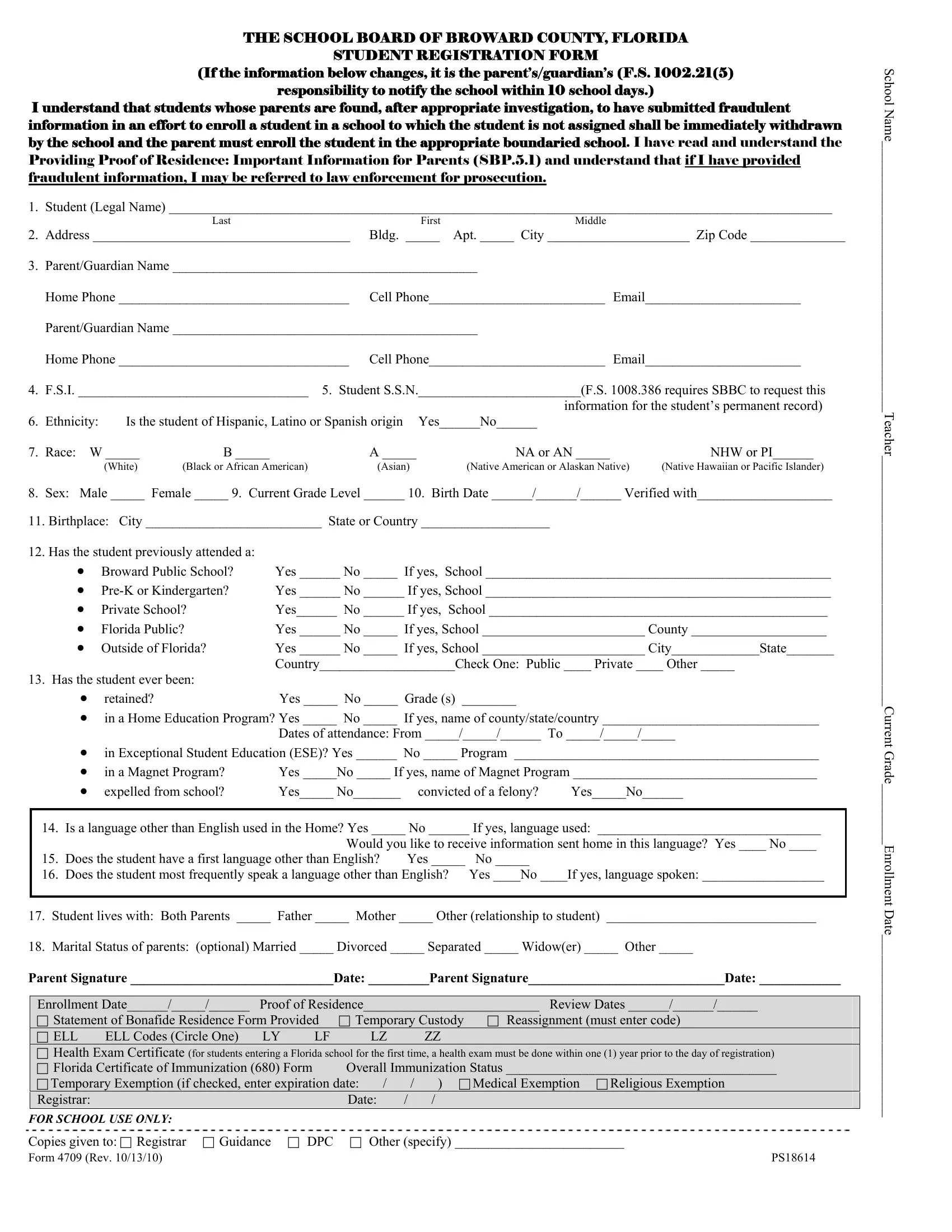
Navigating the intricacies of school registration can be challenging for parents and guardians, but understanding the vital role of specific forms can make the process smoother. The School Board of Broward County, Florida's Student Registration Form, known as Form 4709, serves as a critical tool in enrolling students into the local educational system. This comprehensive form collects essential information, ranging from the student's legal name and residence to prior educational history and health records. It mandates parents or guardians to update the school within ten days should any provided information change, highlighting the importance of accuracy and honesty in the enrollment process. Additionally, it outlines the consequences of submitting fraudulent information, which can lead to immediate withdrawal from the school and possible legal action. The form also encompasses details about the student's ethnicity, race, sex, grade level, birth information, and languages spoken, alongside questions regarding the student's living situation and the marital status of the parents, though the latter is optional. This form not only facilitates the administrative aspect of school registration but also ensures that the educational institution has all the necessary data to support the student's academic journey.
| Question | Answer |
|---|---|
| Form Name | Form 4709 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | NHW, DPC, ZZ, Broward |

THE SCHOOL BOARD OF BROWARD COUNTY, FLORIDA
STUDENT REGISTRATION FORM
(If the information below changes, it is the parent’s/guardian’s (F.S. 1002.21(5)
responsibility to notify the school within 10 school days.)
I understand that students whose parents are found, after appropriate investigation, to have submitted fraudulent information in an effort to enroll a student in a school to which the student is not assigned shall be immediately withdrawn by the school and the parent must enroll the student in the appropriate boundaried school. I have read and understand the Providing Proof of Residence: Important Information for Parents (SBP.5.1) and understand that if I have provided fraudulent information, I may be referred to law enforcement for prosecution.
1. |
Student (Legal Name) __________________________________________________________________________________________________ |
||||||
|
|
|
Last |
First |
Middle |
|
|
2. |
Address ______________________________________ |
Bldg. _____ |
Apt. _____ City _____________________ Zip Code ______________ |
||||
3. |
Parent/Guardian Name _____________________________________________ |
|
|
||||
|
Home Phone __________________________________ |
Cell Phone__________________________ |
Email_______________________ |
||||
|
Parent/Guardian Name _____________________________________________ |
|
|
||||
|
Home Phone __________________________________ |
Cell Phone__________________________ |
Email_______________________ |
||||
4. |
F.S.I. __________________________________ 5. Student S.S.N.________________________(F.S. 1008.386 requires SBBC to request this |
||||||
|
|
|
|
|
information for the student’s permanent record) |
||
6. |
Ethnicity: |
Is the student of Hispanic, Latino or Spanish origin Yes______No______ |
|
|
|||
7. |
Race: W _____ |
B _____ |
A _____ |
NA or AN _____ |
|
NHW or PI______ |
|
|
|
(White) |
(Black or African American) |
(Asian) |
(Native American or Alaskan Native) |
(Native Hawaiian or Pacific Islander) |
|
8.Sex: Male _____ Female _____ 9. Current Grade Level ______ 10. Birth Date ______/______/______ Verified with____________________
11.Birthplace: City __________________________ State or Country ___________________
12. Has the student previously attended a: |
|
|
• |
Broward Public School? |
Yes ______ No _____ If yes, School ___________________________________________________ |
• |
Yes ______ No ______ If yes, School ___________________________________________________ |
|
• |
Private School? |
Yes______ No ______ If yes, School __________________________________________________ |
• |
Florida Public? |
Yes ______ No _____ If yes, School ________________________ County ____________________ |
• |
Outside of Florida? |
Yes ______ No _____ If yes, School ________________________ City_____________State_______ |
|
|
Country____________________Check One: Public ____ Private ____ Other _____ |
13. Has the student ever been: |
|
|
• |
retained? |
Yes _____ No _____ Grade (s) ________ |
•in a Home Education Program? Yes _____ No _____ If yes, name of county/state/country ________________________________
Dates of attendance: From _____/_____/______ To _____/_____/_____
•in Exceptional Student Education (ESE)? Yes ______ No _____ Program _____________________________________________
|
• in a Magnet Program? |
Yes _____No _____ If yes, name of Magnet Program ____________________________________ |
|||
|
• expelled from school? |
Yes_____ No_______ |
convicted of a felony? |
Yes_____No______ |
|
|
|
||||
14. |
Is a language other than English used in the Home? Yes _____ No ______ If yes, language used: _________________________________ |
||||
|
|
Would you like to receive information sent home in this language? Yes ____ No ____ |
|||
15. |
Does the student have a first language other than English? |
Yes _____ |
No _____ |
|
|
16. |
Does the student most frequently speak a language other than English? |
Yes ____No ____If yes, language spoken: __________________ |
|||
|
|
|
|
|
|
17.Student lives with: Both Parents _____ Father _____ Mother _____ Other (relationship to student) _______________________________
18.Marital Status of parents: (optional) Married _____ Divorced _____ Separated _____ Widow(er) _____ Other _____
Parent Signature ______________________________Date: _________Parent Signature_____________________________Date: ____________
Enrollment Date______/_____/______ |
Proof of Residence__________________________ Review Dates ______/______/______ |
|||||||||
Statement of Bonafide Residence Form Provided |
Temporary Custody |
Reassignment (must enter code) |
||||||||
ELL |
ELL Codes (Circle One) |
LY |
LF |
|
LZ |
|
ZZ |
|
|
|
Health Exam Certificate (for students entering a Florida school for the first time, a health exam must be done within one (1) year prior to the day of registration) |
||||||||||
Florida Certificate of Immunization (680) Form |
Overall Immunization Status ________________________________________ |
|||||||||
Temporary Exemption (if checked, enter expiration date: |
/ |
/ |
) |
Medical Exemption |
Religious Exemption |
|||||
Registrar: |
|
|
|
|
Date: |
/ |
/ |
|
|
|
FOR SCHOOL USE ONLY: |
|
|
|
|
|
|
|
|
|
|
Copies given to: Registrar |
Guidance |
DPC |
|
Other (specify) _________________________ |
||||||
Form 4709 (Rev. 10/13/10) |
|
|
|
|
|
|
|
|
PS18614 |
|
School Name________________________________________Teacher_____________________________________Current Grade_________Enrollment Date___________________________