
When you wish to fill out form 5020, you don't need to install any programs - just try our online tool. FormsPal is dedicated to providing you with the absolute best experience with our tool by continuously presenting new functions and enhancements. Our tool has become even more user-friendly thanks to the newest updates! Now, editing PDF forms is a lot easier and faster than ever. Should you be looking to get going, this is what it will require:
Step 1: Just click the "Get Form Button" at the top of this site to access our pdf editing tool. Here you'll find all that is needed to work with your file.
Step 2: After you launch the file editor, you will notice the form made ready to be filled out. In addition to filling in various fields, you might also perform many other actions with the form, that is writing your own words, changing the initial text, adding illustrations or photos, signing the document, and much more.
This document requires some specific details; in order to ensure consistency, please make sure to take heed of the subsequent guidelines:
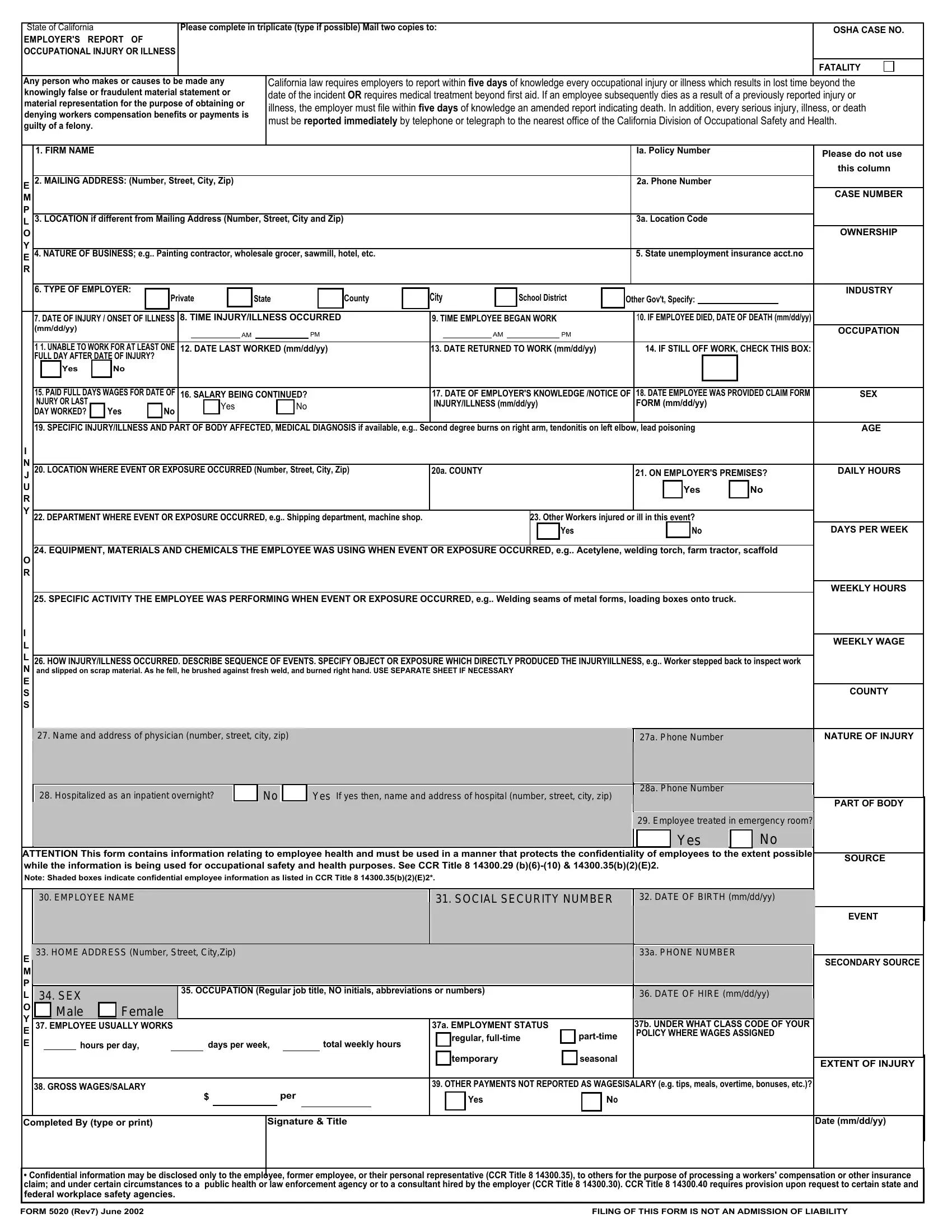
1. While submitting the form 5020, ensure to include all of the needed blanks in their associated part. It will help facilitate the work, enabling your information to be handled without delay and correctly.
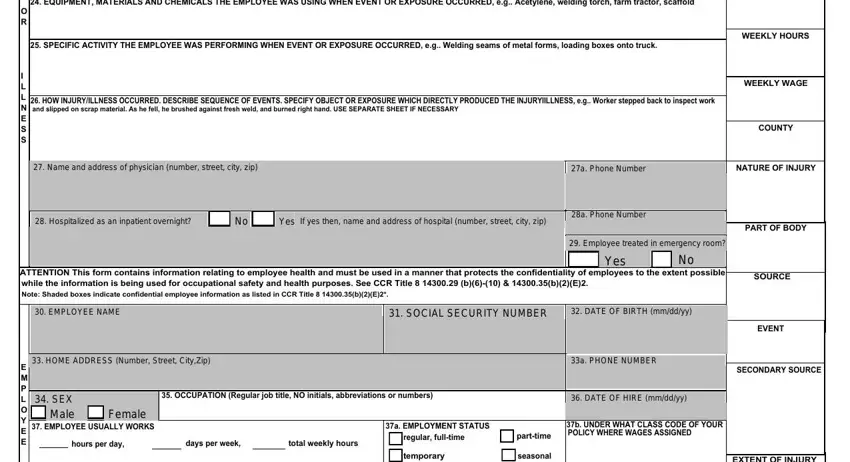
2. The next step would be to submit these particular fields: O R, I L L N E S S, EQUIPMENT MATERIALS AND CHEMICALS, SPECIFIC ACTIVITY THE EMPLOYEE, HOW INJURYILLNESS OCCURRED, WEEKLY HOURS, WEEKLY WAGE, COUNTY, NATURE OF INJURY, PART OF BODY, ATTENTION This form contains, SOURCE, E M P L O Y E E, OCCUPATION Regular job title NO, and EMPLOYEE USUALLY WORKS.
3. This stage is simple - fill out every one of the empty fields in GROSS WAGESSALARY, OTHER PAYMENTS NOT REPORTED AS, Yes, per, Completed By type or print, Signature Title, EXTENT OF INJURY, Date mmddyy, cid Confidential information may, and FORM Rev June FILING OF THIS to conclude this segment.

People who work with this PDF often make errors while completing Date mmddyy in this area. You should definitely read again everything you enter here.
Step 3: Just after double-checking the filled in blanks, click "Done" and you are good to go! Sign up with us right now and immediately obtain form 5020, all set for download. Every last edit made is handily saved , which enables you to customize the document later on if needed. FormsPal provides secure form editor without data record-keeping or distributing. Rest assured that your information is in good hands here!