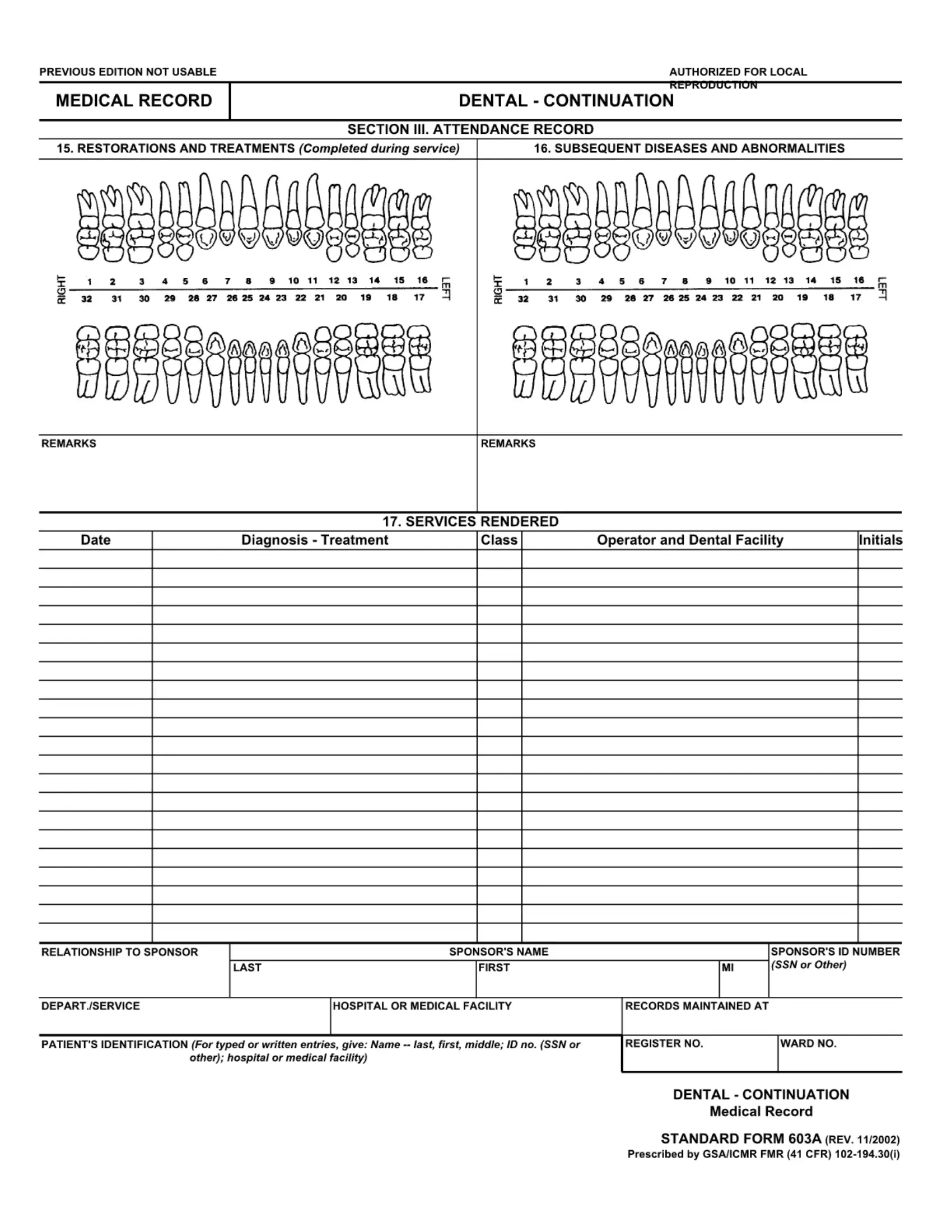
The Standard Form 603-A, commonly known as the Health Record Dental - Continuation, plays a crucial role in the meticulous documentation of an individual's dental care history. Serving as a detailed extension, this form provides a comprehensive platform for recording a myriad of dental care aspects, including but not limited to restorations and treatments received during service, any subsequent diseases and abnormalities encountered, as well as remarks pertinent to the patient's dental health history. Each entry is methodically documented with the patient's symptoms, diagnosis, treatment, the provider's details, and the treatment facility, necessitating a signature to validate each record. Furthermore, the form captures essential patient identification information comprising the patient's name, sex, date of birth, and relationship to the sponsor, alongside their service component and departure status, underscoring the form's significance in maintaining an organized chronology of dental care for individuals, especially those connected with service. The Form 603-A, approved for use by the General Services Administration and the Information Resources Management Service, ensures that dental care professionals have a structured and reliable record-keeping tool, illustrating its pivotal role in the continuous care and monitoring of dental health within diverse populations.
| Question | Answer |
|---|---|
| Form Name | Form 603 A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | standard 603a, 1975 standard form, standard form record, form 603a |
STANDARD FORM
HEALTH RECORD
DENTAL - CONTINUATION
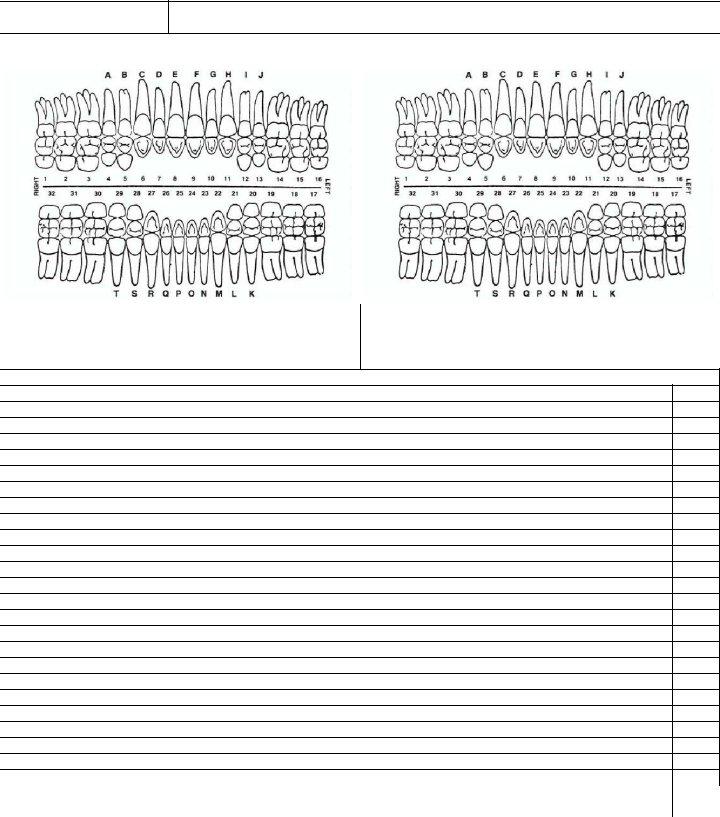
SECTION II. CHRONOLOGICAL RECORD OF DENTAL CARE |
PAGE: |
8. RESTORATIONS AND TREATMENTS (Completed during service) |
9. SUBSEQUENT DISEASES AND ABNORMALITIES |
|
|
|
|
REMARKS |
REMARKS |
10. SERVICES PROVIDED
DATE |
SYMPTOMS, DIAGNOSIS, TREATMENT, PROVIDER, TREATMENT FACILITY (Sign each entry) |
|
|
CLASS
PATIENT'S IDENTIFICATION (Use this Space for Mechanical |
PATIENT'S NAME (Last, First, Middle Initial) |
|
|
SEX |
|
Imprint) |
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
RELATIONSHIP TO SPONSOR |
COMPONENT STATUS |
DEPART SERVICE |
|
|
|
|
|
|
|
|
SPONSOR'S NAME |
|
|
RANK/GRADE |
|
|
|
|
|
|
|
|
SSN OR IDENTIFICATION NO. |
|
ORGANIZATION |
|
|
|
|
|
|
||
|
EXCEPTION TO SF 603A |
|
STANDARD FORM 603A |
||
|
APPROVED BY GSA/IRMS |
|
GSA/ICMR |
||
|
|
|
|
FIRMR (41 CFR) |
|
ADOBE PROFESSIONAL 8.0
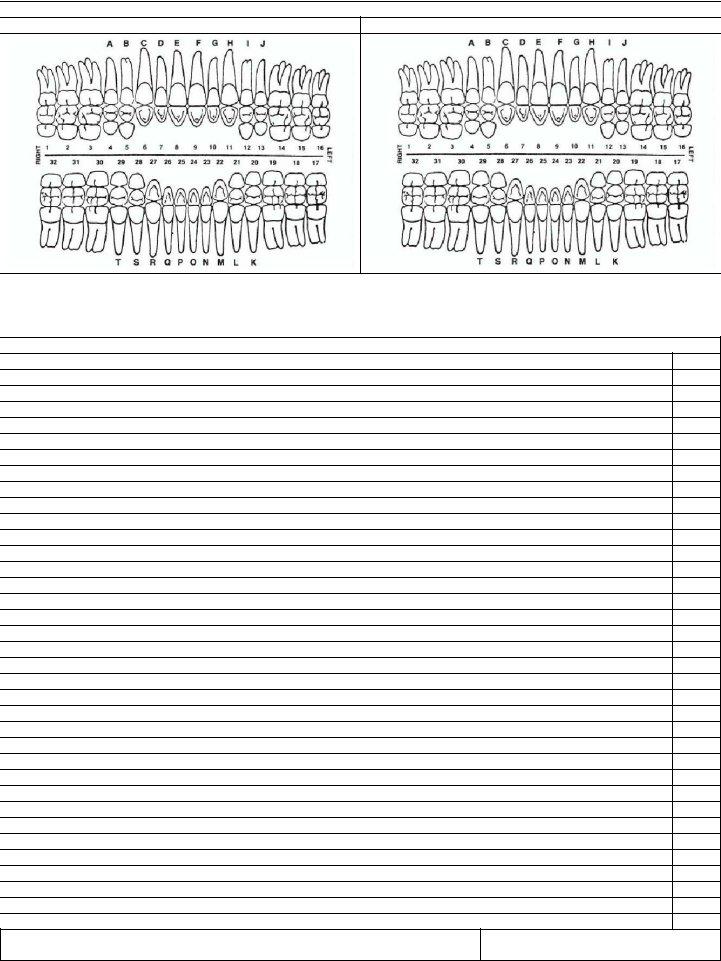
SECTION II. CHRONOLOGICAL RECORD OF DENTAL CARE |
PAGE: |
8. RESTORATIONS AND TREATMENTS (Completed during service)
9. SUBSEQUENT DISEASES AND ABNORMALITIES
REMARKS |
REMARKS |
|
|
10. SERVICES PROVIDED
DATE |
SYMPTOMS, DIAGNOSIS, TREATMENT, PROVIDER, TREATMENT FACILITY (Sign each entry) |
|
|
CLASS
PATIENT'S NAME:
SF 603A (SIDE 2)
SSN: