
 or C) on form.
or C) on form.










 box(es)
box(es)
 K-12
K-12 are complete for 7
are complete for 7 and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.
and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.


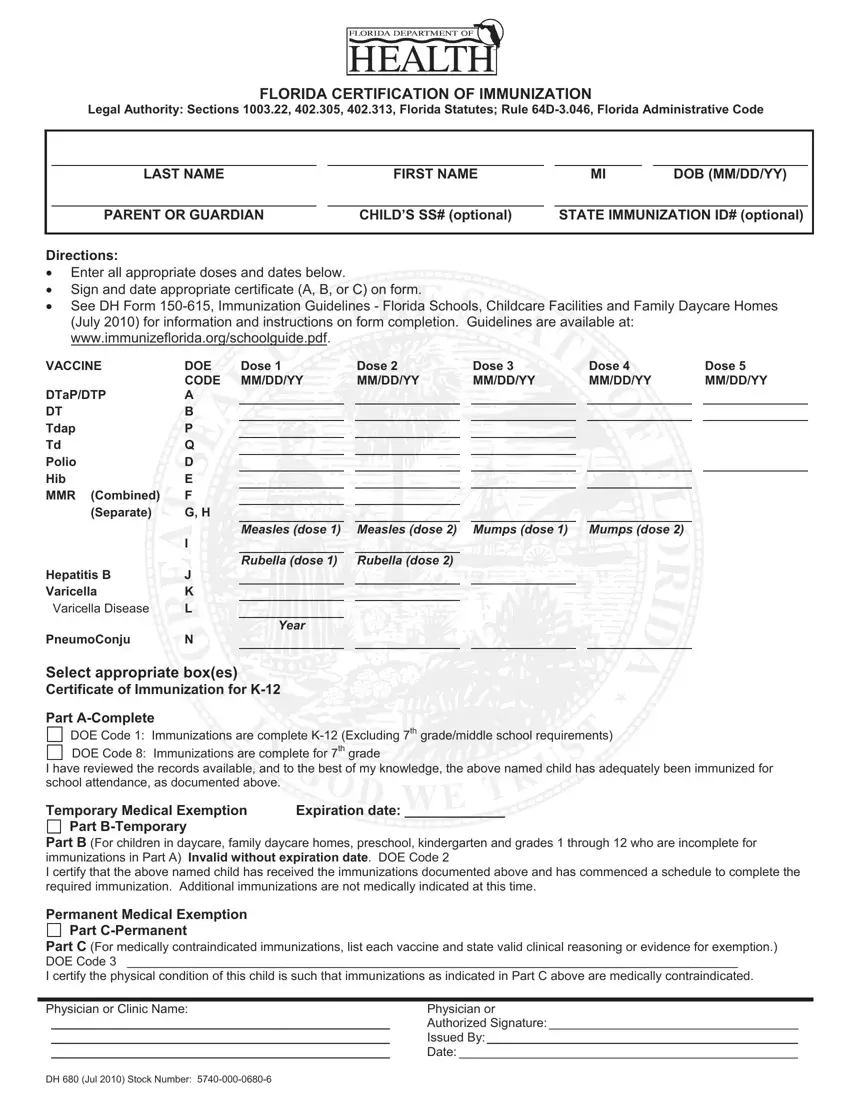
Healthcare providers like doctors or clinic staff fill out and sign the DH 680 form, and parents or guardians usually just provide basic details and turn it in.
If you use FormsPal, your private information isn’t stored, so your data stays safe.
Child’s Personal Info
Write the last name, first name, middle initial, and date of birth. Add the name of the parent or guardian, then include the child’s Social Security number and State Immunization ID.
Clinics and schools use these details to match records within the Florida Department of Health system, especially when a child enrolls for the first time or transfers to an additional grade.
Vaccine Information
Move to the vaccine table and enter all immunization doses the child has received. Write each vaccination date in the correct column under the matching vaccine name and code.
The form lists vaccines such as DTaP, Polio, MMR, Hepatitis B, Varicella, and pneumococcal conjugate, along with protection against illnesses like measles, diphtheria, and tetanus. Some vaccines require three doses, while others may require four doses (it depends on the child’s age and timing).
Certification Section
Choose the certificate that matches the child’s immunization status.
• Part A - Complete: Mark when the child has received all required vaccines.• Part B - Temporary: Use this option if the child still needs additional doses but has started the required schedule.
• Part C - Permanent: Complete this section when medical conditions prevent certain vaccinations. List each exempt vaccine and provide valid clinical reasoning (not covering a religious exemption).
Only one section should apply, and the healthcare provider must complete and sign it.

Provider Certification Details
This part includes the physician or clinic name, authorized signature, issuing provider details, and the date of completion.
The provider’s signature confirms that the immunization information matches medical records and meets Florida health requirements.
