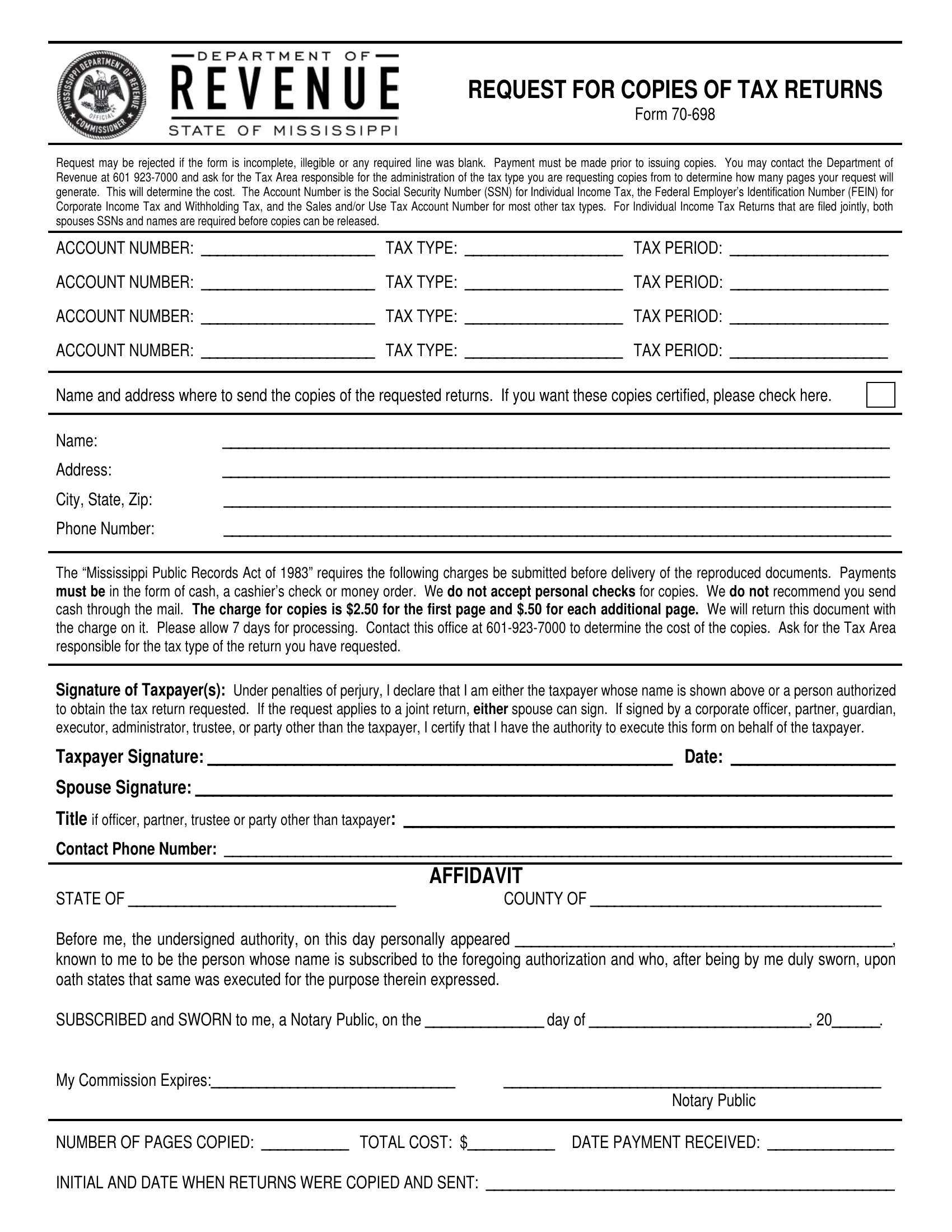
When individuals or entities need to obtain copies of their tax returns, they often turn to Form 70-698, a critical document that facilitates the request for duplicates from the Department of Revenue. This procedure, while seemingly straightforward, encompasses specific prerequisites such as the completion and legibility of the form, along with the necessary identification of the tax type, tax period, and account numbers, which vary depending on whether the tax concerns individual income, corporate income, withholding, or sales/use tax. Furthermore, for married couples filing jointly, details of both spouses are required. An aspect often underlined is the due cost for acquiring these copies—initially set at $2.50 for the first page with an additional fifty cents for each subsequent page. This process not only necessitates awareness of the associated fees but also underscores the importance of confirming the exact amount with the responsible tax area before proceeding. The form further emphasizes adherence to the Mississippi Public Records Act of 1983 regarding the remittance of fees and restrictions on payment methods. Additionally, the document stipulates the necessity of an affidavit, accompanies payment instructions, and lays out the conditions under which a request may be rejected, showcasing the legal formally underscoring the right to access personal tax return information. Equally important is the certification by the requester, asserting their identity as the taxpayer or a duly authorized person, a safeguard meant to ensure the confidentiality and security of sensitive financial information.
| Question | Answer |
|---|---|
| Form Name | Form 70 698 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | forms_70 698 ms form 70 698 |
REQUEST FOR COPIES OF TAX RETURNS
Form
Request may be rejected if the form is incomplete, illegible or any required line was blank. Payment must be made prior to issuing copies. You may contact the Department of Revenue at 601
ACCOUNT NUMBER: ______________________ |
TAX TYPE: ____________________ |
TAX PERIOD: ____________________ |
ACCOUNT NUMBER: ______________________ |
TAX TYPE: ____________________ |
TAX PERIOD: ____________________ |
ACCOUNT NUMBER: ______________________ |
TAX TYPE: ____________________ |
TAX PERIOD: ____________________ |
ACCOUNT NUMBER: ______________________ |
TAX TYPE: ____________________ |
TAX PERIOD: ____________________ |
|
|
|
Name and address where to send the copies of the requested returns. If you want these copies certified, please check here.
Name: |
_____________________________________________________________________________________ |
Address: |
_____________________________________________________________________________________ |
City, State, Zip: |
_____________________________________________________________________________________ |
Phone Number: |
_____________________________________________________________________________________ |
The “Mississippi Public Records Act of 1983” requires the following charges be submitted before delivery of the reproduced documents. Payments must be in the form of cash, a cashier’s check or money order. We do not accept personal checks for copies. We do not recommend you send cash through the mail. The charge for copies is $2.50 for the first page and $.50 for each additional page. We will return this document with the charge on it. Please allow 7 days for processing. Contact this office at
Under penalties of perjury, I declare that I am either the taxpayer whose name is shown above or a person authorized to obtain the tax return requested. If the request applies to a joint return, either spouse can sign. If signed by a corporate officer, partner, guardian, executor, administrator, trustee, or party other than the taxpayer, I certify that I have the authority to execute this form on behalf of the taxpayer.
Taxpayer Signature: ______________________________________________________ Date: ___________________
Spouse Signature: _________________________________________________________________________________
Title if officer, partner, trustee or party other than taxpayer: _________________________________________________________
Contact Phone Number: _____________________________________________________________________________________
|
AFFIDAVIT |
STATE OF __________________________________ |
COUNTY OF _____________________________________ |
Before me, the undersigned authority, on this day personally appeared ________________________________________________,
known to me to be the person whose name is subscribed to the foregoing authorization and who, after being by me duly sworn, upon oath states that same was executed for the purpose therein expressed.
SUBSCRIBED and SWORN to me, a Notary Public, on the _______________ day of ____________________________, 20______.
My Commission Expires:_______________________________ |
________________________________________________ |
|
Notary Public |
|
|
NUMBER OF PAGES COPIED: ___________ TOTAL COST: $___________ DATE PAYMENT RECEIVED: ________________
INITIAL AND DATE WHEN RETURNS WERE COPIED AND SENT: ____________________________________________________