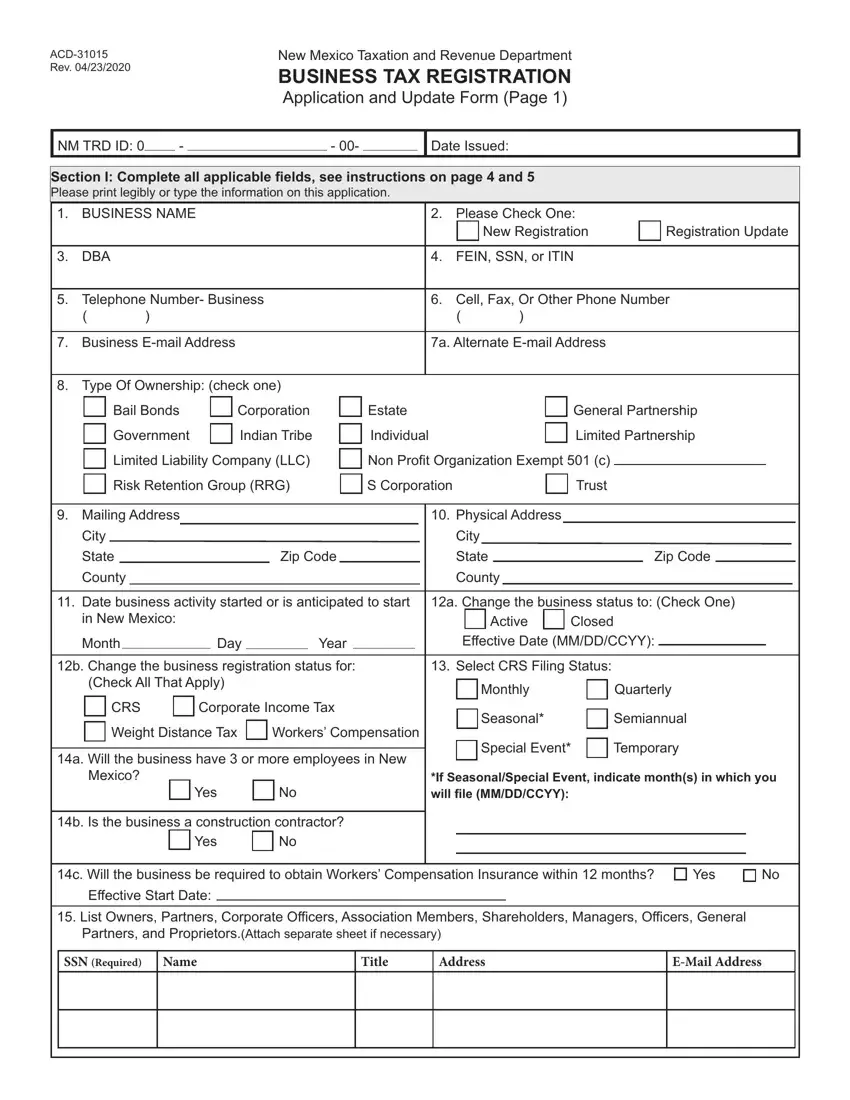
Embarking on the journey of business ownership or maintaining the compliance of an existing business in New Mexico necessitates familiarity with the ACD-31015 form. Officially titled the Business Tax Registration Application and Update Form, it serves as a critical step for entities engaging in commercial activities within the state. This form, as of its latest revision on April 23, 2020, is a comprehensive document designed to facilitate the registration and updating process for businesses with the New Mexico Taxation and Revenue Department. It encompasses a broad range of fields including business identification details, the type of ownership, contact information, the nature of the business, and specific tax program affiliations. Furthermore, the form contains sections dedicated to special tax programs, oil and gas activities, insurance premium taxes, and more, reflecting the varied regulatory landscape businesses must navigate. The ACD-31015 form stands as a pivotal tool for businesses to ensure their compliance with state taxation requirements, encompassing initial registration and any subsequent updates reflecting changes in the business's status or operational scope. Entities are guided through this regulatory maze with detailed instructions provided within the form, ensuring clarity and compliance in their business operations.
| Question | Answer |
|---|---|
| Form Name | Form Acd 31015 |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | new mexico form acd 31015, state of new mexico form acd 31015, nm acd 31015, how to new mexico acd 31015 |
