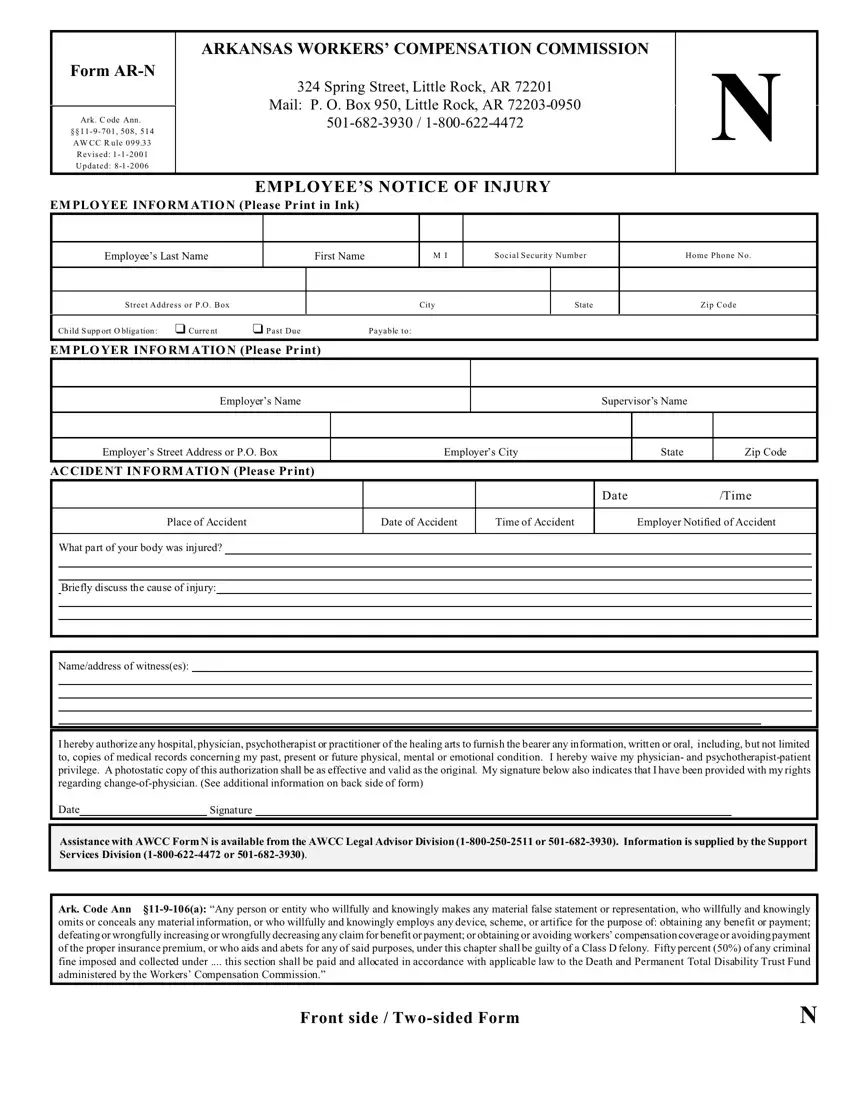
The Form AR-N, as prescribed by the Arkansas Workers' Compensation Commission, is a critical document for employees who have sustained injuries at work. Located at 324 Spring Street, Little Rock, AR, with updates as recent as 2006, this form facilitates the notification process for employees to report workplace injuries to their employers. It collects detailed information about the employee, the employer, and the accident itself, including the time, place, and cause of the injury, along with witness details. The form also plays a pivotal role in enabling access to workers' compensation benefits by ensuring a documented account of the injury is reported in a timely manner, as stipulated under Ark. Code Ann. §§11-9-701 among other sections. Moreover, it outlines the employee's right to choose or change their physician for treatment, under certain conditions, reflecting the importance of medical care and treatment continuity post-injury. The inclusion of a clause about potential felony charges for anyone attempting to fraudulently benefit from workers' compensation highlights the seriousness with which the state of Arkansas treats the integrity of its workers' compensation system. Through its comprehensive design, the Form AR-N serves not only as a tool for reporting injuries but also as a guide for injured employees navigating the complex process of claiming workers' compensation benefits.
| Question | Answer |
|---|---|
| Form Name | Form Ar N |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | arkansas form ar p, arkansas school choice form 2020, ar workers comp state form in spanish, arkansas n online |
