
You could complete ies without difficulty by using our PDFinity® editor. The editor is constantly maintained by our staff, acquiring handy functions and growing to be greater. This is what you'd want to do to start:
Step 1: Open the PDF doc in our editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: As soon as you access the online editor, you will get the document all set to be filled in. Besides filling out different blanks, it's also possible to perform some other things with the PDF, specifically writing any textual content, modifying the original text, inserting illustrations or photos, signing the PDF, and much more.
This document will require specific data to be typed in, therefore be sure you take your time to type in what is asked:
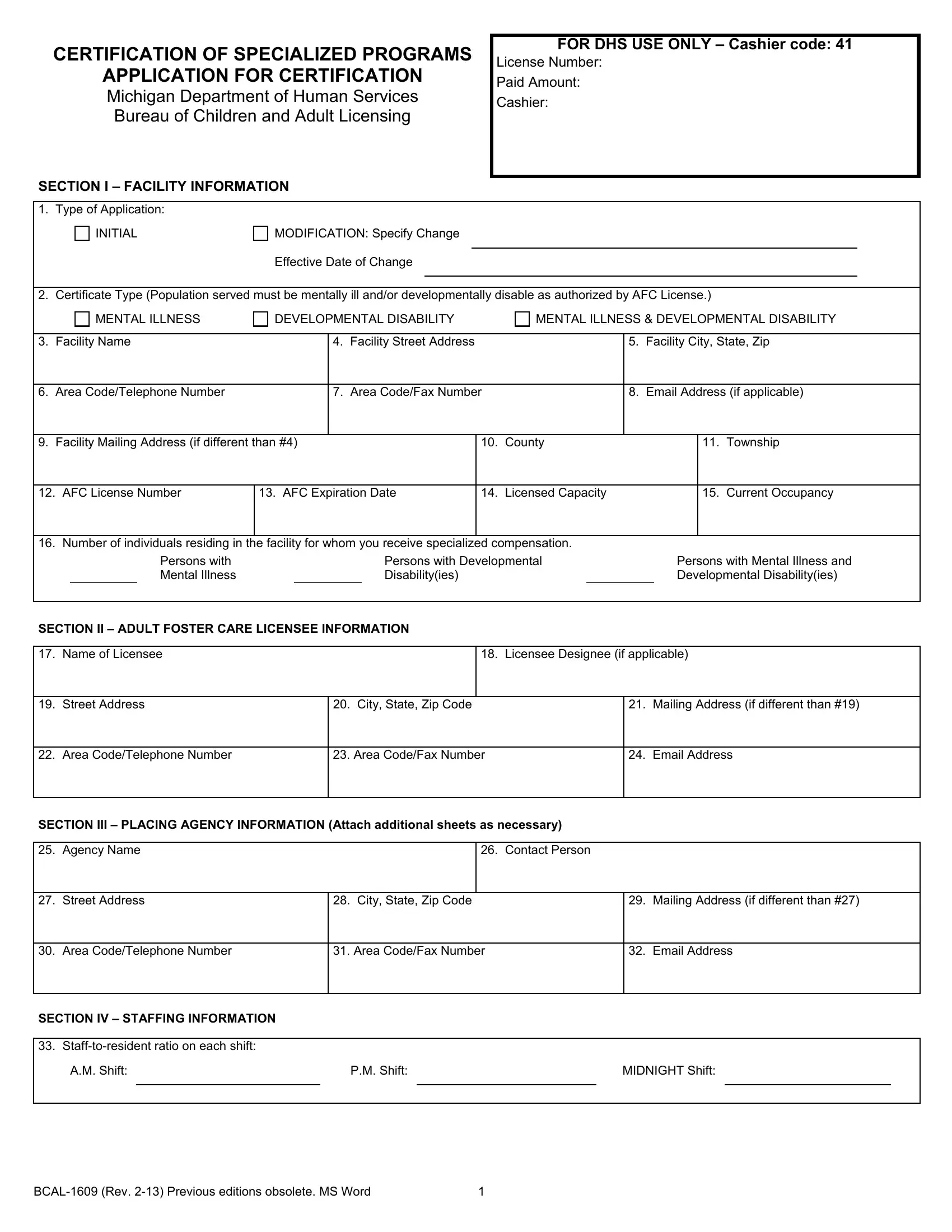
1. While completing the ies, make certain to include all important blanks within its relevant area. It will help to expedite the process, enabling your information to be processed promptly and correctly.
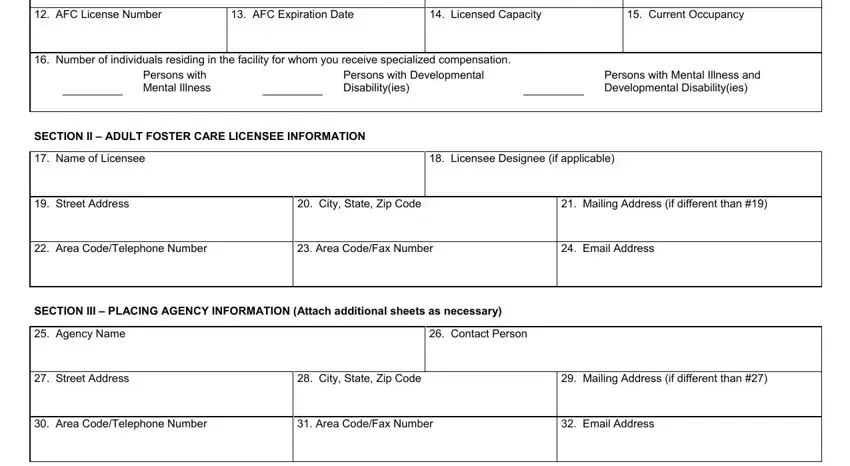
2. Once the last section is done, you're ready include the required specifics in AFC License Number, AFC Expiration Date, Licensed Capacity, Current Occupancy, Number of individuals residing in, Persons with Mental Illness, Persons with Developmental, Persons with Mental Illness and, Disabilityies, Developmental Disabilityies, SECTION II ADULT FOSTER CARE, Name of Licensee, Street Address, Licensee Designee if applicable, and City State Zip Code so you're able to proceed to the third step.
3. In this specific part, examine Stafftoresident ratio on each, AM Shift, PM Shift, MIDNIGHT Shift, and BCAL Rev Previous editions. All these are required to be filled in with highest focus on detail.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Specialized Program Description - to proceed further in your process!
5. The last step to submit this PDF form is crucial. You'll want to fill in the displayed form fields, and this includes The applicant certified that the, Licensee or Licensee Designee, Date Signed, Authority, PA PA, Completion Mandatory, Penalty, Certification will not be issued, Department of Human Services DHS, and BCAL Rev Previous editions, before using the pdf. Failing to do this may give you an incomplete and possibly invalid document!
People who work with this form often make errors when completing The applicant certified that the in this area. You need to reread everything you type in right here.
Step 3: Ensure that the information is accurate and just click "Done" to conclude the task. Acquire the ies after you sign up at FormsPal for a 7-day free trial. Conveniently gain access to the pdf document within your personal account, with any modifications and changes conveniently saved! FormsPal is focused on the privacy of all our users; we ensure that all personal information used in our tool remains protected.