
You may fill out optional effortlessly using our online PDF tool. The editor is constantly upgraded by us, acquiring handy features and growing to be greater. This is what you'd need to do to get started:
Step 1: Just click the "Get Form Button" at the top of this site to see our pdf file editing tool. This way, you will find everything that is necessary to fill out your file.
Step 2: After you launch the PDF editor, you will see the form prepared to be completed. Apart from filling in various blanks, you could also perform various other things with the file, including adding your own textual content, changing the original textual content, inserting illustrations or photos, signing the PDF, and more.
Completing this form needs care for details. Make sure each blank field is completed properly.
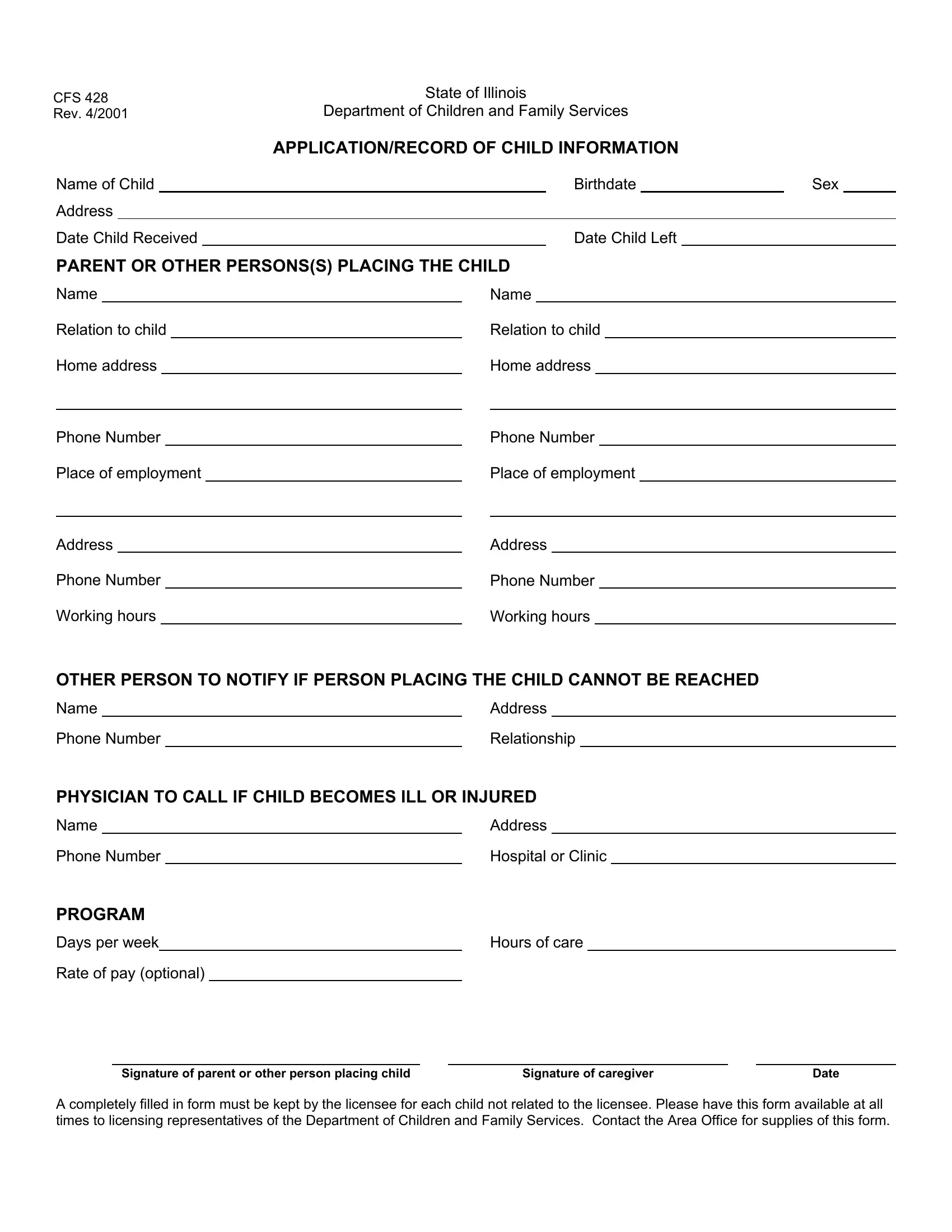
1. The optional will require certain details to be inserted. Be sure the subsequent blank fields are completed:
2. The subsequent step is usually to complete the next few blanks: Phone Number, Working hours, Phone Number, Working hours, OTHER PERSON TO NOTIFY IF PERSON, Name, Phone Number, Address, Relationship, PHYSICIAN TO CALL IF CHILD BECOMES, Name, Phone Number, PROGRAM, Days per week, and Rate of pay optional.
Always be extremely careful while filling in Rate of pay optional and Phone Number, because this is where many people make some mistakes.
3. In this stage, examine Signature of parent or other, A completely filled in form must, Signature of caregiver, and Date. Each of these must be completed with highest precision.
4. It is time to begin working on this fourth part! In this case you will get these If the child has any of the, Medical problems, Physical handicaps, Restrictions for playoutdoors, Restrictions for playindoors, Allergies, Food likes, and Food dislikes form blanks to do.
5. When you draw near to the last sections of this form, you'll notice several more things to complete. Particularly, Fears, Does the child take a nap, Is the child toilet trained, Time, Length, Does the child have special names, Does the child regularly take, If so what kind and directions, If the child is an infant what are, Time, Amount, Temperature, Diaper changes, Powder, and Ointment must be filled out.
Step 3: Prior to moving on, it's a good idea to ensure that all form fields are filled out right. Once you believe it's all good, click “Done." Find your optional when you sign up for a 7-day free trial. Conveniently access the form within your personal cabinet, along with any edits and changes all preserved! FormsPal provides protected document tools with no personal information record-keeping or any sort of sharing. Feel comfortable knowing that your details are secure here!