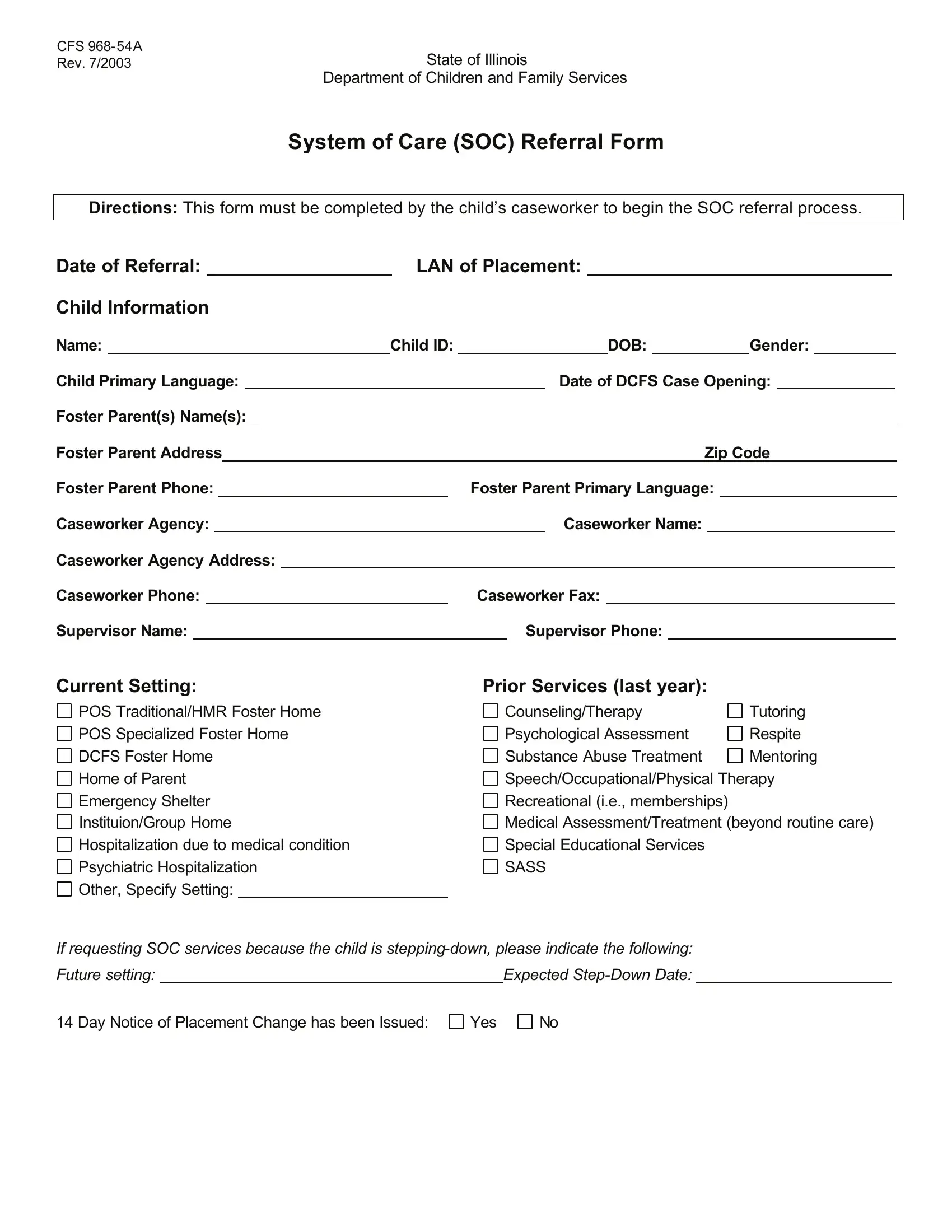
In the realm of child welfare, the completion and submission of specific forms stand as critical steps toward ensuring that children in need receive appropriate care and support. Among these forms, the CFS 968-54A, revised in July 2003 by the State of Illinois Department of Children and Family Services, plays a pivotal role in the System of Care (SOC) referral process. Designed to be filled out by a child's caseworker, this form initiates the procedure for referring a child to the SOC program. It captures extensive information, including the date of the referral, placement details, child's personal information such as name, ID, date of birth, gender, primary language, and the opening date of their Department of Children and Family Services (DCFS) case. Additionally, it delves into foster parent details, the caseworker's agency and supervisor information, the child's current setting, a record of services provided in the last year, and the specifics regarding any step-down in service. Moreover, the form includes sections for describing the issues prompting the referral and the desired outcomes from the SOC, complemented by a checklist for further information needed and a space for caseworker and supervisor signatures. This comprehensive approach ensures a thorough understanding of the child's situation and needs, facilitating targeted support through the SOC system.
| Question | Answer |
|---|---|
| Form Name | Form Cfs 968 54A |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | CFS_968 54A_System_of_C are_(SOC)_Refer ral_Form_(Filla ble) illinois soc referral form |
CFS
Rev. 7/2003State of Illinois
Department of Children and Family Services
System of Care (SOC) Referral Form
Directions: This form must be completed by the child’s caseworker to begin the SOC referral process.
Date of Referral: |
|
|
LAN of Placement: |
|
|
|
|
|
|
|||||||||||||||||||
Child Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Name: |
|
Child ID: |
|
|
|
|
|
DOB: |
|
Gender: |
|
|
|
|||||||||||||||
Child Primary Language: |
|
|
|
|
|
|
Date of DCFS Case Opening: |
|
|
|
||||||||||||||||||
Foster Parent(s) Name(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Foster Parent Address |
|
|
|
|
|
|
|
|
|
|
Zip Code |
|
|
|||||||||||||||
Foster Parent Phone: |
|
|
|
|
|
Foster Parent Primary Language: |
|
|
|
|
|
|
||||||||||||||||
Caseworker Agency: |
|
|
|
|
|
|
Caseworker Name: |
|
|
|
|
|
|
|||||||||||||||
Caseworker Agency Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Caseworker Phone: |
|
|
|
|
Caseworker Fax: |
|
|
|
|
|
|
|||||||||||||||||
Supervisor Name: |
|
|
|
|
|
Supervisor Phone: |
|
|
|
|
|
|
||||||||||||||||
Current Setting: |
|
|
|
Prior Services (last year): |
|
|
|
|
|
|||||||||||||||||||
POS Traditional/HMR Foster Home POS Specialized Foster Home DCFS Foster Home
Home of Parent Emergency Shelter Instituion/Group Home Hospitalization due to medical condition Psychiatric Hospitalization
Other, Specify Setting:
Counseling/Therapy |
Tutoring |
Psychological Assessment |
Respite |
Substance Abuse Treatment |
Mentoring |
Speech/Occupational/Physical Therapy Recreational (i.e., memberships)
Medical Assessment/Treatment (beyond routine care) Special Educational Services
SASS
If requesting SOC services because the child is
Future setting: |
|
Expected |
14 Day Notice of Placement Change has been Issued:
Yes
No
Briefly describe the presenting issues that have caused you to seek assistance from SOC, and state specifically what you are seeking from SOC (pertinent documentation may also be attached). Include why the referral is being made now:
Caseworker Signature: |
|
|
Date: |
|
Supervisor Signature: |
|
|
|
Date: |
SOC Provider: |
|
|
|
Child Name: |
|
|
FP Phone Number(s) |
|
Best Time to Call |
|
|||
FP Work: |
Beginning: |
am/pm |
End: |
am/pm |
||
FP Home: |
Beginning: |
am/pm |
End: |
am/pm |
||
FP Other: |
Beginning: |
am/pm |
End: |
am/pm |
||
Child ID:
Check Available Days
S M T W T F S
S M T W T F S
S M T W T F S
Additional Information Requested
θDCFS Client Service Plan
θPsychological Assessments
θAdditional Collateral Information
θCounseling
θInitial Social History/Comprehensive Assessment/Addendums
θRelease(s) of Information (needed for release of confidential information)
θOther
For SOC Staff Use Only: * Additional information collected directly from referring caseworker (i.e., type,
frequency of services, etc.):
SOC Disposition
θ
θ
Acceptance of the referral
Refer back to DCFS or foster care agency: Reason(s) case is being referred back to DCFS or foster
care agency, including recommendations for service/intervention:
SOC Worker Signature: |
|
Date: |
*After making a disposition decision, the SOC provider must fax this completed form to the referring caseworker within two days of receiving the referral.