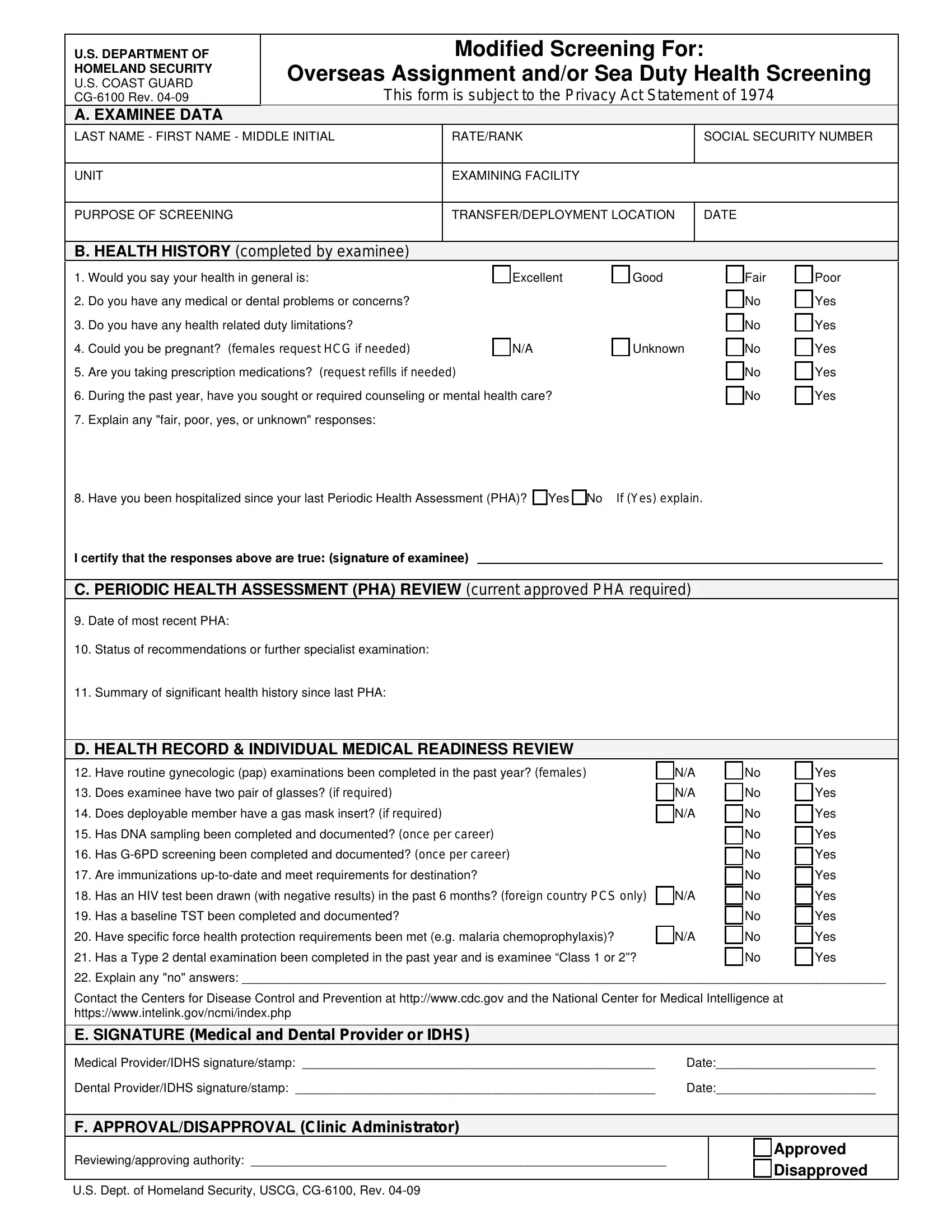
When members of the U.S. Coast Guard are preparing for overseas assignments or sea duty, they must complete a comprehensive health screening process, which is documented on a crucial form known as the CG-6100. Revised in April 2009, this form serves as a central piece in ensuring the readiness and well-being of personnel who are about to embark on missions that may place them in physically demanding or challenging environments. The CG-6100 form is a detailed document that collects information ranging from personal health history to current medical readiness, including any limitations that might affect the member's ability to serve overseas or at sea. The form prompts individuals to provide detailed information on their general health status, any medical or dental concerns, possible pregnancies, prescription medications, mental health care in the past year, and hospitalizations since their last Periodic Health Assessment (PHA). Moreover, it requires a review of the individual's health records and a series of evaluations to ensure they meet the specific health requirements for their destined location, including up-to-date immunizations, HIV testing, and dental examinations. By meticulously compiling this information, the CG-6100 form supports the U.S. Coast Guard's commitment to maintaining a force that is both prepared and medically fit, ensuring that its members are well-equipped to meet the challenges of their assignments while also protecting their health and safety.
| Question | Answer |
|---|---|
| Form Name | Form Cg 6100 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cg 6100 form, 1974, HCG, chemoprophylaxis |
U.S. DEPARTMENT OF |
|
|
Modified Screening For: |
|
|
||
HOMELAND SECURITY |
Overseas Assignment and/or Sea Duty Health Screening |
|
|||||
U.S. COAST GUARD |
|
||||||
|
This form is subject to the Privacy Act Statement of 1974 |
|
|||||
|
|
||||||
|
A. EXAMINEE DATA |
|
|
|
|
|
|
LAST NAME - FIRST NAME - MIDDLE INITIAL |
|
RATE/RANK |
|
SOCIAL SECURITY NUMBER |
|
||
|
|
|
|
|
|
|
|
UNIT |
|
|
EXAMINING FACILITY |
|
|
||
|
|
|
|
|
|
||
PURPOSE OF SCREENING |
|
|
TRANSFER/DEPLOYMENT LOCATION |
|
DATE |
|
|
|
|
|
|
|
|
|
|
B. HEALTH HISTORY (completed by examinee)
1. |
Would you say your health in general is: |
Excellent |
Good |
|
Fair |
Poor |
|
|
|||||
2. |
Do you have any medical or dental problems or concerns? |
|
|
|
No |
Yes |
|
|
|||||
3. |
Do you have any health related duty limitations? |
|
|
|
No |
Yes |
|
|
|||||
4. |
Could you be pregnant? (females request HCG if needed) |
N/A |
Unknown |
No |
Yes |
|
|
||||||
5. |
Are you taking prescription medications? (request refills if needed) |
|
|
|
No |
Yes |
|
|
|||||
6. |
During the past year, have you sought or required counseling or mental health care? |
|
|
No |
Yes |
|
|
||||||
7. |
Explain any "fair, poor, yes, or unknown" responses: |
|
|
|
|
|
|
|
|
||||
8. |
Have you been hospitalized since your last Periodic Health Assessment (PHA)? Yes No |
If (Yes) explain. |
|
|
|
|
|
||||||
|
I certify that the responses above are true: (signature of examinee) |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. PERIODIC HEALTH ASSESSMENT (PHA) REVIEW (current approved PHA required) |
|
|
|
|
|
||||||
9. |
Date of most recent PHA: |
|
|
|
|
|
|
|
|
||||
10. |
Status of recommendations or further specialist examination: |
|
|
|
|
|
|
|
|
||||
11. |
Summary of significant health history since last PHA: |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
D. HEALTH RECORD & INDIVIDUAL MEDICAL READINESS REVIEW |
|
|
|
|
|
|
|
||||
12. |
Have routine gynecologic (pap) examinations been completed in the past year? (females) |
|
N/A |
No |
Yes |
|
|
||||||
13. |
Does examinee have two pair of glasses? (if required) |
|
|
N/A |
No |
Yes |
|
|
|||||
14. |
Does deployable member have a gas mask insert? (if required) |
|
|
N/A |
No |
Yes |
|
|
|||||
15. |
Has DNA sampling been completed and documented? (once per career) |
|
|
|
No |
Yes |
|
|
|||||
16. |
Has |
|
|
|
No |
Yes |
|
|
|||||
17. |
Are immunizations |
|
|
|
No |
Yes |
|
|
|||||
18. |
Has an HIV test been drawn (with negative results) in the past 6 months? (foreign country PCS only) |
N/A |
No |
Yes |
|
|
|||||||
19. |
Has a baseline TST been completed and documented? |
|
|
|
No |
Yes |
|
|
|||||
20. |
Have specific force health protection requirements been met (e.g. malaria chemoprophylaxis)? |
|
N/A |
No |
Yes |
|
|
||||||
21. |
Has a Type 2 dental examination been completed in the past year and is examinee “Class 1 or 2”? |
|
No |
Yes |
|
|
|||||||
22. |
Explain any "no" answers: _____________________________________________________________________________________________ |
|
|
||||||||||
|
Contact the Centers for Disease Control and Prevention at http://www.cdc.gov and the National Center for Medical Intelligence at |
|
|
||||||||||
|
https://www.intelink.gov/ncmi/index.php |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
E. SIGNATURE (Medical and Dental Provider or IDHS) |
|
|
|
|
|
|
|
|
|||
|
Medical Provider/IDHS signature/stamp: ___________________________________________________ |
Date:_______________________ |
|
|
|||||||||
|
Dental Provider/IDHS signature/stamp: ____________________________________________________ |
Date:_______________________ |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
F. APPROVAL/DISAPPROVAL (Clinic Administrator) |
|
|
|
|
|
|
|
|
|||
|
Reviewing/approving authority: ____________________________________________________________ |
|
|
Approved |
|
|
|||||||
|
|
|
Disapproved |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
U.S. Dept. of Homeland Security, USCG,