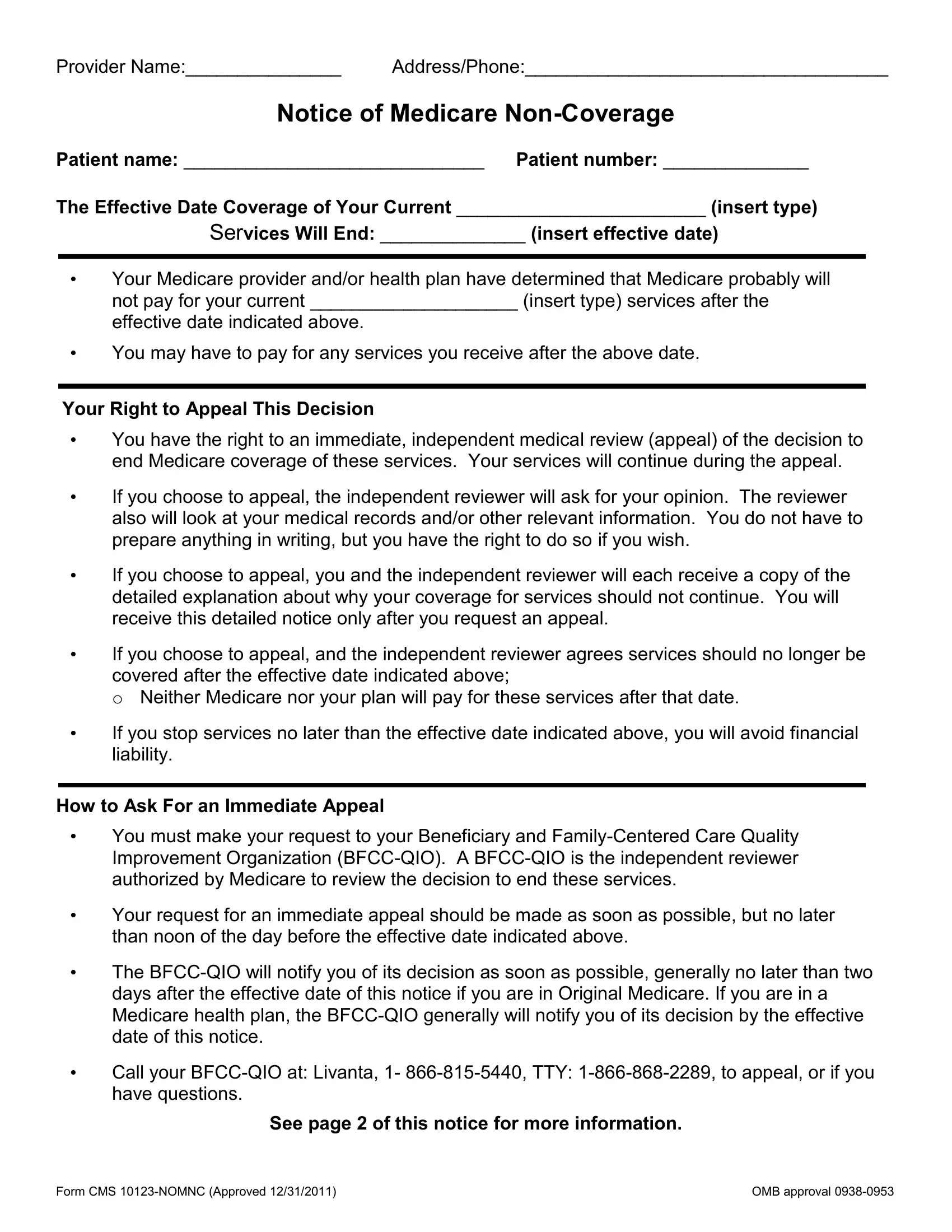
Navigating the healthcare landscape can often feel like traversing a complex maze, especially when it comes to understanding the ins and outs of Medicare coverage. At the heart of this maze lies the CMS 10123 NOMNC form, a critical document for patients receiving Medicare benefits. This form serves as a notice from either the patient's Medicare provider or health plan, indicating that Medicare is likely to stop paying for the current services being received after a specified date. It's a document that essentially tells patients that the financial coverage they were relying on for specific health services is about to end, and it lays out their rights to challenge this decision. The form outlines the importance of initiating an appeal through an immediate, independent medical review if the patient disagrees with the cessation of services. During this appeal process, services will continue, ensuring that patients are not left without necessary care while their case is being reviewed. Highlighting the steps to request an appeal, it mentions contacting the Beneficiary and Family-Centered Care Quality Improvement Organization (BFCC-QIO) before a set deadline to avoid potential financial liability for services received after coverage ends. For those who miss the initial appeal deadline, the form also provides information on other avenues for contesting the decision, depending on whether the individual is part of Original Medicare or a Medicare health plan. Complete with contact information for the appeal process and instructions for how to proceed, the CMS 10123 NOMNC form is designed to inform and empower patients at a critical juncture in their care journey.
| Question | Answer |
|---|---|
| Form Name | Form CMS 10123-NOMNC |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | nomnc form 2020 pdf, form cms 10123 nomnc 2020, form cms 10123 nomnc, cms 10123 nomnc form fillable |