Our top developers worked hard to design the PDF editor we are excited to present to you. The application permits you to instantly fill in home health care plan template and will save you your time. You just need to stick to this procedure.
Step 1: The initial step will be to hit the orange "Get Form Now" button.
Step 2: At this point, it is possible to change the home health care plan template. Our multifunctional toolbar enables you to add, get rid of, modify, highlight, and conduct other sorts of commands to the content and fields within the form.
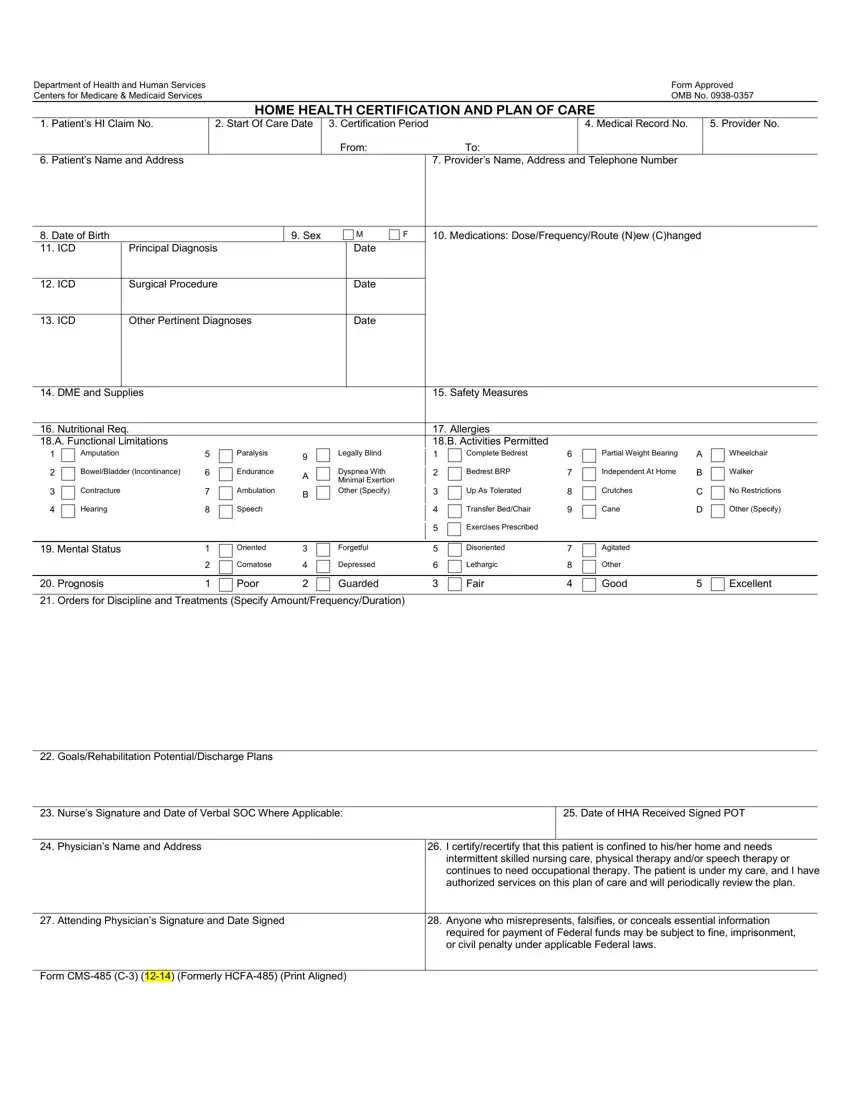
Fill in the home health care plan template PDF and provide the information for each section:
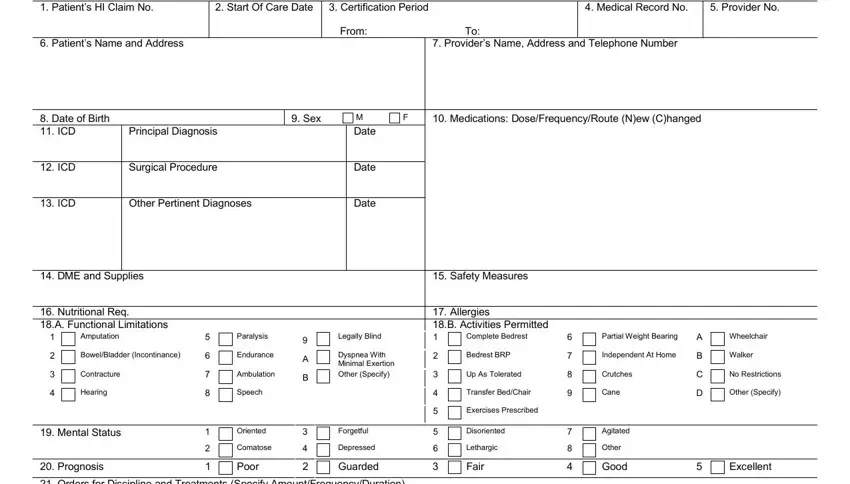
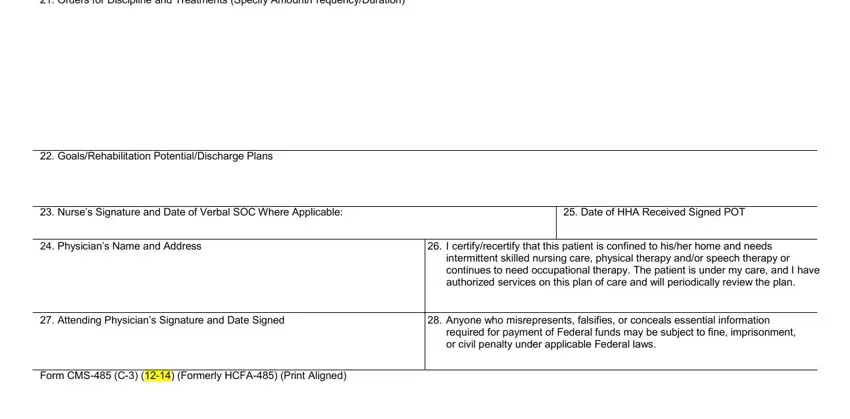
Type in the details in the Orders for Discipline and, GoalsRehabilitation, Nurses Signature and Date of, Date of HHA Received Signed POT, Physicians Name and Address, I certifyrecertify that this, intermittent skilled nursing care, Attending Physicians Signature, Anyone who misrepresents, required for payment of Federal, and Form CMS C Formerly HCFA Print field.
It's essential to record particular information in the area According to the Paperwork.
Step 3: Select the "Done" button. Now it's easy to upload the PDF document to your device. Besides, you can deliver it through email.
Step 4: Prepare copies of the template. This is going to prevent potential future problems. We do not read or display the information you have, thus be certain it is safe.
