
 Employing Unit With Eligible Employees – Section 702.6
Employing Unit With Eligible Employees – Section 702.6
You can easily complete documents with the help of our PDF editor. Updating the de1378n file is a breeze in case you keep to the next steps:
Step 1: Search for the button "Get Form Here" on this webpage and click it.
Step 2: Once you've got entered the editing page de1378n, you will be able to discover all of the functions available for the document at the top menu.
The next parts are what you are going to complete to obtain the finished PDF form.
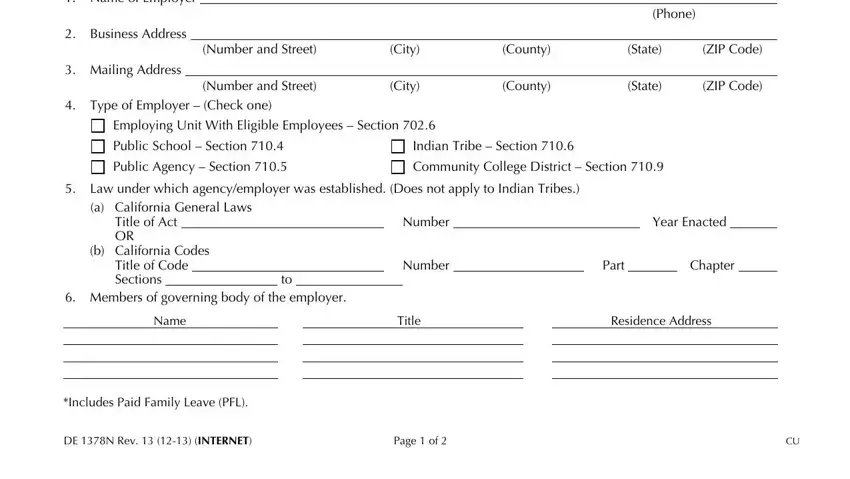
Fill out the Name of Employer, Business Address, Mailing Address, Number and Street, Number and Street, City, City, County, State, ZIP Code, County, State, ZIP Code, Phone, and Type of Employer Check one fields with any data that can be asked by the software.
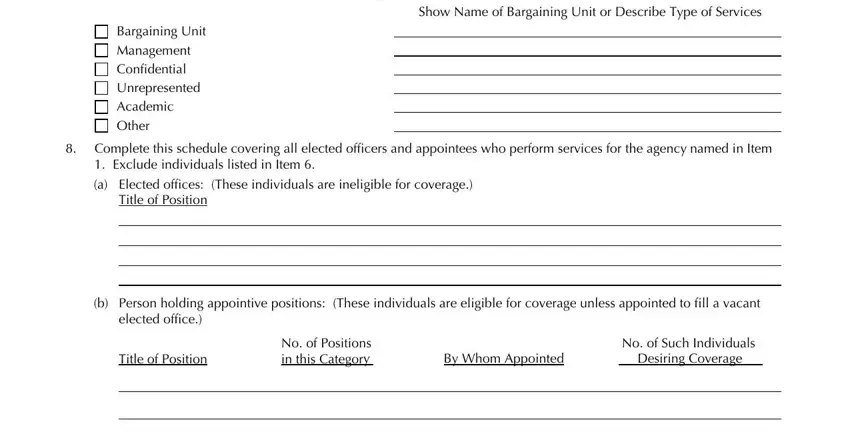
Write down the crucial information in This application covers employees, Show Name of Bargaining Unit or, Bargaining Unit Management, Complete this schedule covering, Title of Position, b Person holding appointive, elected office, Title of Position, No of Positions in this Category, By Whom Appointed, and No of Such Individuals Desiring area.
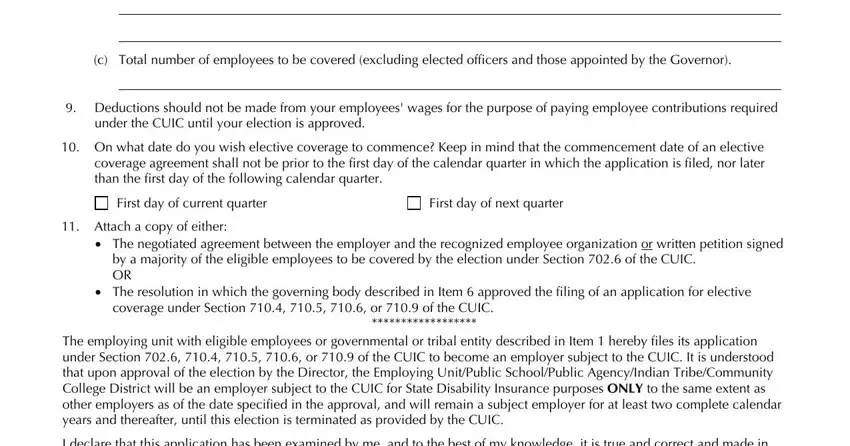
The c Total number of employees to be, Deductions should not be made, under the CUIC until your election, On what date do you wish elective, First day of current quarter, First day of next quarter, Attach a copy of either, The negotiated agreement between, by a majority of the eligible, The resolution in which the, coverage under Section or of, The employing unit with eligible, and I declare that this application segment should be applied to write down the rights or obligations of both parties.
Finalize by checking the next sections and typing in the appropriate details: I declare that this application, This declaration must be signed by, Signed Signed Signed, Date Date Date, DE N Rev INTERNET, and Page of.

Step 3: If you're done, click the "Done" button to transfer the PDF file.
Step 4: To prevent yourself from any kind of problems in the long run, you should generate at the very least a couple of copies of the document.
