
By using the online PDF editor by FormsPal, you're able to complete or edit Form Dhcs 9113 right here. To make our editor better and less complicated to work with, we continuously implement new features, taking into consideration suggestions coming from our users. It merely requires just a few simple steps:
Step 1: Just click the "Get Form Button" above on this page to start up our pdf editor. This way, you'll find all that is necessary to work with your file.
Step 2: With the help of our handy PDF tool, you can actually do more than just complete forms. Edit away and make your documents look perfect with customized text incorporated, or optimize the original content to excellence - all that accompanied by the capability to add any photos and sign the PDF off.
Filling out this document usually requires care for details. Ensure that all necessary blank fields are filled out accurately.
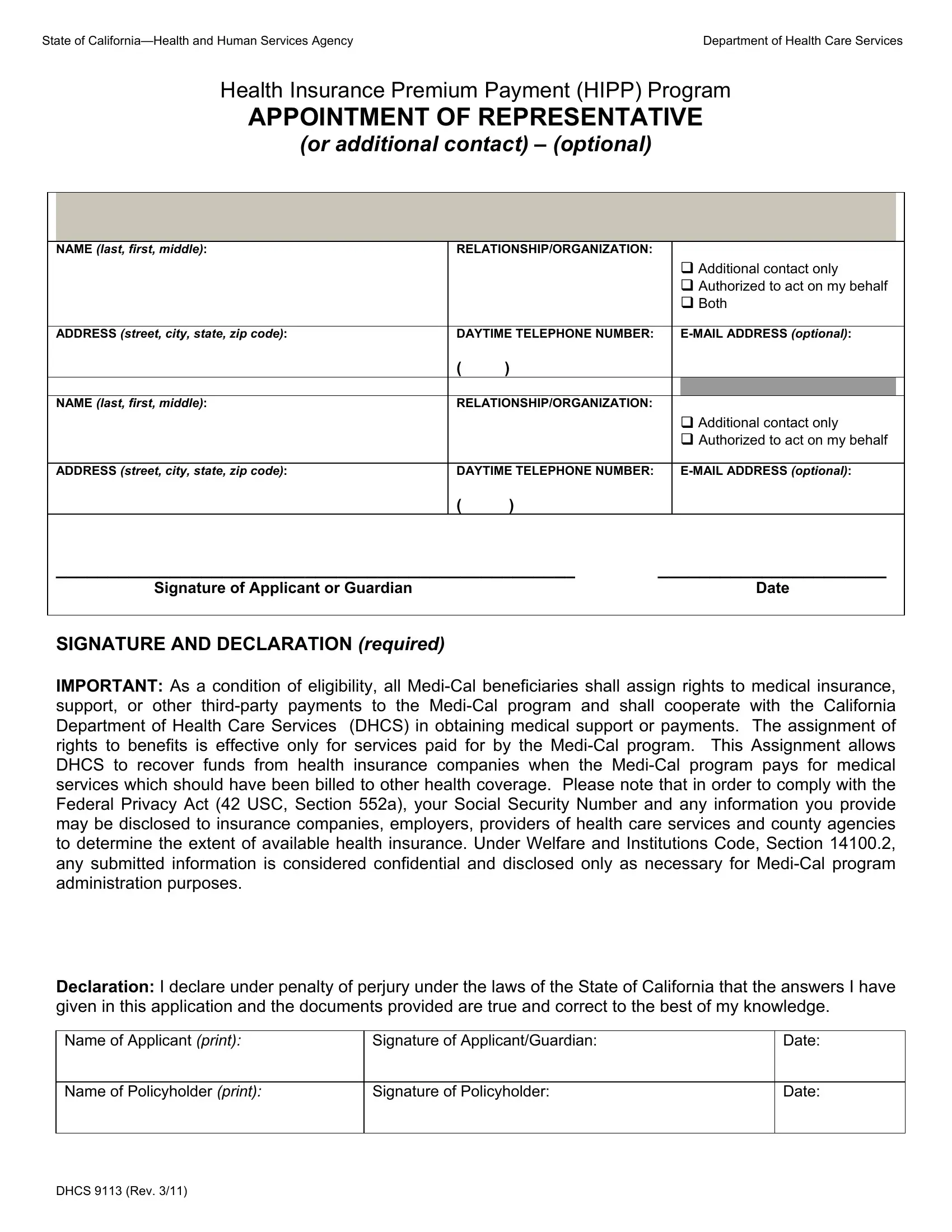
1. The Form Dhcs 9113 requires specific details to be inserted. Ensure that the following fields are filled out:
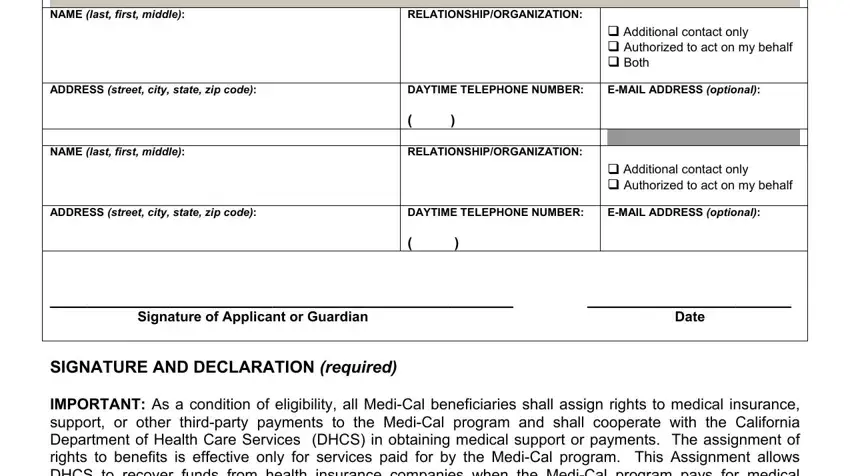
2. Once this array of fields is completed, you have to add the needed specifics in ADDRESS street city state zip code, Name of Applicant print, Signature of ApplicantGuardian, Name of Policyholder print, Signature of Policyholder, Date, Date, and DHCS Rev in order to progress further.
It is possible to make errors while filling out the Date, consequently be sure to look again prior to deciding to submit it.
Step 3: As soon as you've reread the details in the fields, click on "Done" to finalize your form at FormsPal. Go for a 7-day free trial option with us and acquire direct access to Form Dhcs 9113 - which you can then begin using as you would like from your FormsPal account. We do not share or sell the details you provide when filling out documents at our site.