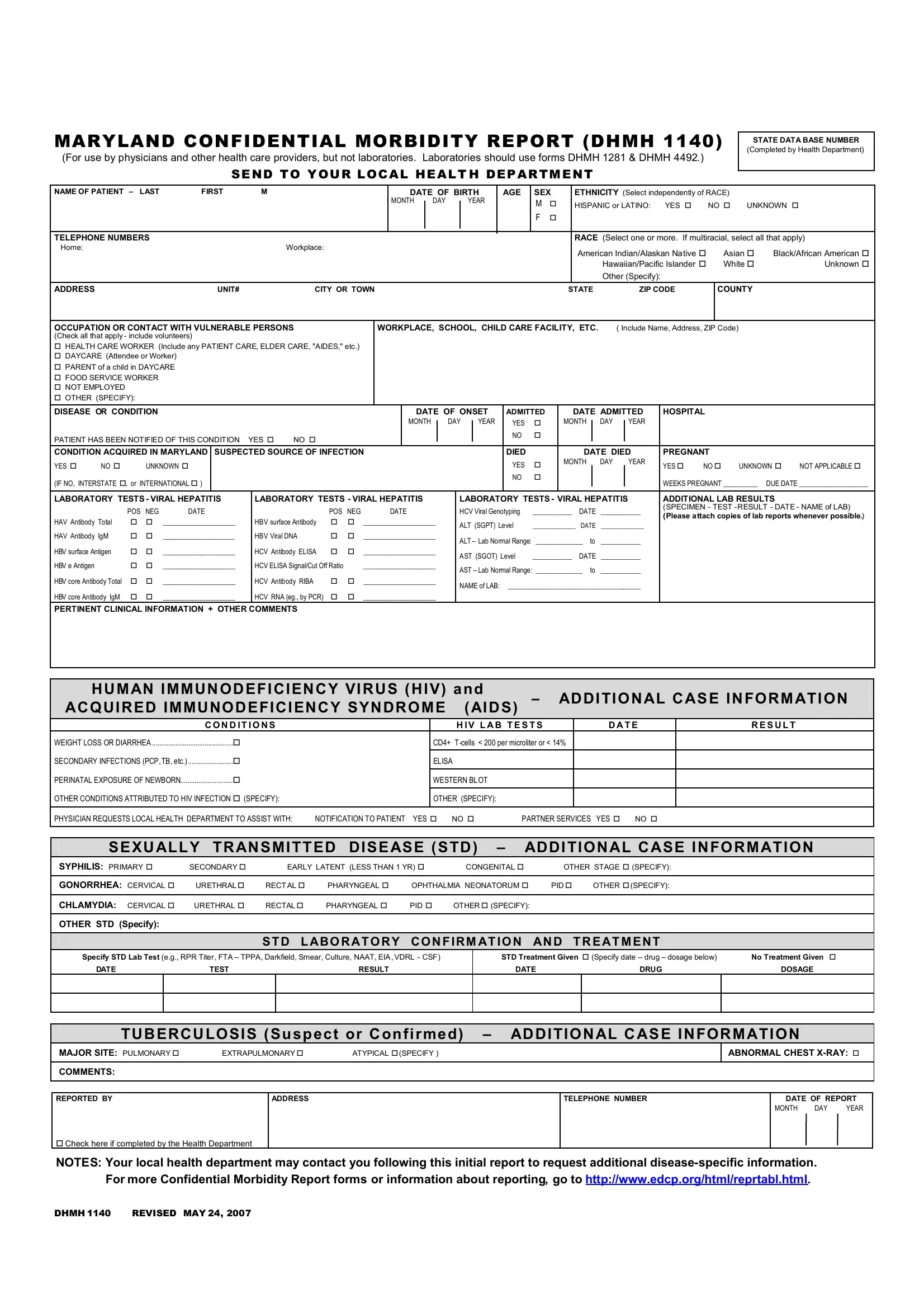
The Maryland Confidential Morbidity Report (DHMH 1140) serves a crucial role in safeguarding public health by facilitating the structured communication of morbidity information from healthcare providers, excluding laboratories, to local health departments. This report caters to a wide spectrum of medical conditions, emphasizing the importance of detailed patient information, including demographics such as name, birth date, ethnicity, and race, as well as contact details. It stretches beyond basic identifiers, requiring specific data on patients' occupation, potential contact with vulnerable populations, and the disease or condition reported—including onset, hospital admissions, and if applicable, death. Furthermore, the form intricately details laboratory tests, especially focusing on viral hepatitis and other conditions like HIV/AIDS, to ascertain precise medical circumstances. Noteworthy, it incorporates sections for sexually transmitted diseases (STDs) and tuberculosis, underlining the broad scope of conditions that healthcare providers must report. Additionally, the DHMH 1140 form facilitates a critical component of patient care and public health management by enabling providers to request assistance from local health departments in notifying patients and offering partner services. Revised last on May 24, 2007, this form stands as a testament to Maryland's commitment to monitoring and managing public health through detailed and comprehensive reporting mechanisms.
| Question | Answer |
|---|---|
| Form Name | Form Dhmh 1140 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ASE, ATI, dhmh 1140, PID |
MARYLAND CONFIDENTIAL MORBIDITY REPORT (DHMH 1140)
(For use by physicians and other health care providers, but not laboratories. Laboratories should use forms DHMH 1281 & DHMH 4492.)
SEND TO YOUR LOCAL HEALT H DEPARTMENT
STATE DATA BASE NUMBER (Completed by Health Department)
NAME OF PATIENT – LAST |
FIRST |
M |
|
DATE OF BIRTH |
AGE |
SEX |
|
ETHNICITY (Select independently of RACE) |
|
||||||
|
|
|
|
MONTH |
DAY |
YEAR |
|
M |
|
|
HISPANIC or LATINO: YES |
NO UNKNOWN |
|||
|
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE NUMBERS |
|
|
|
|
|
|
|
|
|
|
RACE (Select one or more. If multiracial, select all that apply) |
||||
Home: |
|
Workplace: |
|
|
|
|
|
|
|
|
American Indian/Alaskan Native |
|
Asian |
Black/African American |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Hawaiian/Pacific Islander |
|
White |
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify): |
|
|
|
ADDRESS |
UNIT# |
CITY OR TOWN |
|
|
|
|
|
|
|
STATE |
ZIP CODE |
|
COUNTY |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
OCCUPATION OR CONTACT WITH VULNERABLE PERSONS |
WORKPLACE, SCHOOL, CHILD CARE FACILITY, ETC. |
( Include Name, Address, ZIP Code) |
|
||||||||||||
(Check all that apply - include volunteers) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEALTH CARE WORKER (Include any PATIENT CARE, ELDER CARE, "AIDES," etc.)
DAYCARE (Attendee or Worker)
PARENT of a child in DAYCARE
FOOD SERVICE WORKER
NOT EMPLOYED
OTHER (SPECIFY):
DISEASE OR CONDITION |
|
DATE OF ONSET |
ADMITTED |
DATE ADMITTED |
HOSPITAL |
||||||||||
|
|
|
MONTH |
|
DAY |
|
YEAR |
YES |
|
MONTH |
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
|
||||||||
PATIENT HAS BEEN NOTIFIED OF THIS CONDITION YES |
NO |
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONDITION ACQUIRED IN MARYLAND |
SUSPECTED SOURCE OF INFECTION |
DIED |
|
DATE DIED |
PREGNANT |
|
|
|||||
YES |
NO |
UNKNOWN |
|
YES |
|
MONTH DAY YEAR |
YES |
NO |
UNKNOWN |
NOT APPLICABLE |
||
|
|
|
|
|||||||||
(IF NO, INTERSTATE , or INTERNATIONAL ) |
|
NO |
|
|
|
|
WEEKS PREGNANT __________ DUE DATE ____________________ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
LABORATORY TESTS - VIRAL HEPATITIS |
LABORATORY TESTS - VIRAL HEPATITIS |
LABORATORY TESTS - VIRAL HEPATITIS |
ADDITIONAL LAB RESULTS |
|||||||||
|
POS |
NEG |
DATE |
|
POS |
NEG |
DATE |
HCV Viral Genotyping |
___________ |
DATE |
___________ |
(SPECIMEN - TEST |
|
|
(Please attach copies of lab reports whenever possible.) |
||||||||||
HAV Antibody Total |
|
|
_____________________ |
HB V surface Antibody |
|
|
_____________________ |
|
|
|
|
|
ALT (SGPT) Level |
______________ |
DATE |
______________ |
|
||||||||
|
|
|
|
|
|
|
|
|
||||
HAV Antibody IgM |
|
|
_____________________ |
HB V Viral DNA |
|
|
_____________________ |
ALT – Lab Normal Range: _____________ to |
___________ |
|
||
|
|
|
|
|
|
|
|
|
||||
HBV surface Antigen |
|
|
_____________________ |
HCV Antibody ELISA |
|
|
_____________________ |
A ST (SGOT) Level |
___________ |
DATE |
___________ |
|
|
|
|
|
|
|
|
|
|
||||
HBV e Antigen |
|
|
_____________________ |
HCV ELISA Signal/Cut Off Ratio |
|
_____________________ |
AST – Lab Normal Range : _____________ to |
___________ |
|
|||
|
|
|
|
|
|
|
|
|
||||
HBV core Antibody Total |
|
|
_____________________ |
HCV Antibody RIBA |
|
|
_____________________ |
NAME of LAB: _____________________________________ |
|
|||
|
|
|
|
|
|
|
|
|
||||
HBV core Antibody IgM |
|
|
_____________________ |
HCV RNA (eg., by PCR) |
|
|
_____________________ |
|
|
|
|
|
PERTINENT CLINICAL INFORMATION + OTHER COMMENTS
HUMAN IMMUNODEFICIENCY VIRUS (HIV) and
ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS) – ADDITIONAL CASE INFORMATION
|
C O N D IT I O N S |
|
H IV L A B T E S T S |
|
D A T E |
R E S U L T |
|
WEIGHT LOSS OR DIARRHEA |
|
|
CD4+ T |
|
|
|
|
......................... |
|
|
|
|
|
|
|
SECONDARY INFECTIONS (PCP, TB, etc.) |
|
ELISA |
|
|
|
|
|
............................. |
|
|
|
|
|
|
|
PERINATAL EXPOSURE OF NEWBORN |
|
WESTERN BL OT |
|
|
|
|
|
OTHER CONDITIONS ATTRIBUTED TO HIV INFECTION (SPECIFY): |
|
|
|
|
|
|
|
|
OTHER (SPECIFY): |
|
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
PHYSICIAN REQUESTS LOCAL HEALTH DEPARTMENT TO ASSIST WITH: |
NOTIFICATION TO PATIENT YES NO |
PARTNER SERVICES |
YES NO |
|
|||
|
|
|
|
|
|
|
|
SEXUALLY TRANSMITTED DISEASE (STD) – ADDITIONAL CASE INFORMATION
SYPHILIS: PRIMARY |
SECONDARY |
EARLY LATENT (LESS THAN 1 YR) |
CONGENITAL |
OTHER STAGE (SPECIFY): |
|||
|
|
|
|
|
|
|
|
GONORRHEA: CERVICAL |
URETHRAL |
RECT AL |
PHARYNGEAL |
OPHTHALMIA NEONATORUM |
PID |
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
|
CHLAMYDIA: CERVICAL |
URETHRAL |
RECTAL |
PHARYNGEAL |
PID |
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
|
|
OTHER STD (Specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STD L ABO RATORY CONFIRM AT ION AND TREAT MENT
Specify STD Lab Test (e.g., RPR Titer, FTA – TPPA, Darkfield, Smear, Culture, NAAT, EIA,VDRL - CSF)
DATE |
TEST |
RESULT |
STD Treatment Given (Specify date – drug – dosage below) |
No Treatment Given |
|
DATE |
DRUG |
DOSAGE |
TUBERCULOSIS (Suspect or Confirmed) – ADDITIONAL CASE INFORMATION
MAJOR SITE: PULMONARY |
EXTRAPULMONARY |
ATYPICAL (SPECIFY ) |
ABNORMAL CHEST
COMMENTS:
REPORTED BY
ADDRESS
TELEPHONE NUMBER
DATE OF REPORT
MONTH DAY YEAR
Check here if completed by the Health Department
NOTES: Your local health department may contact you following this initial report to request additional
DHMH 1140 REVISED MAY 24, 2007