The DHS 390 form, an integral document from the Michigan Department of Human Services, serves as an application for a wide range of adult services intended to enhance the well-being and independence of applicants. This comprehensive application process is designed to address the needs of adults seeking assistance to remain in their homes, require help with personal care and housekeeping, or need protection due to being in danger. Additionally, it encompasses services for adults who cannot stay in their homes anymore by facilitating the search for adult foster care, homes for the aged, or nursing facilities, as well as providing support for those already residing in such institutions. The form is also tailored to assist physically disabled adults in acquiring special adaptive equipment or home modifications to live more independently. Significantly, the DHS 390 form stands as a testament to the commitment of the Michigan Department of Human Services to ensure that every individual is treated with fairness, dignity, and without discrimination, emphasizing the rights of applicants to a prompt review process, non-discrimination, and the ability to appeal decisions. Furthermore, responsibilities of the applicants, such as providing accurate information and promptly reporting changes in their situation, are clearly outlined, ensuring a mutual understanding between the Department and the service beneficiaries.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 390 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Sate, NONDISCRIMINATION, dhs 390 form, TTD |
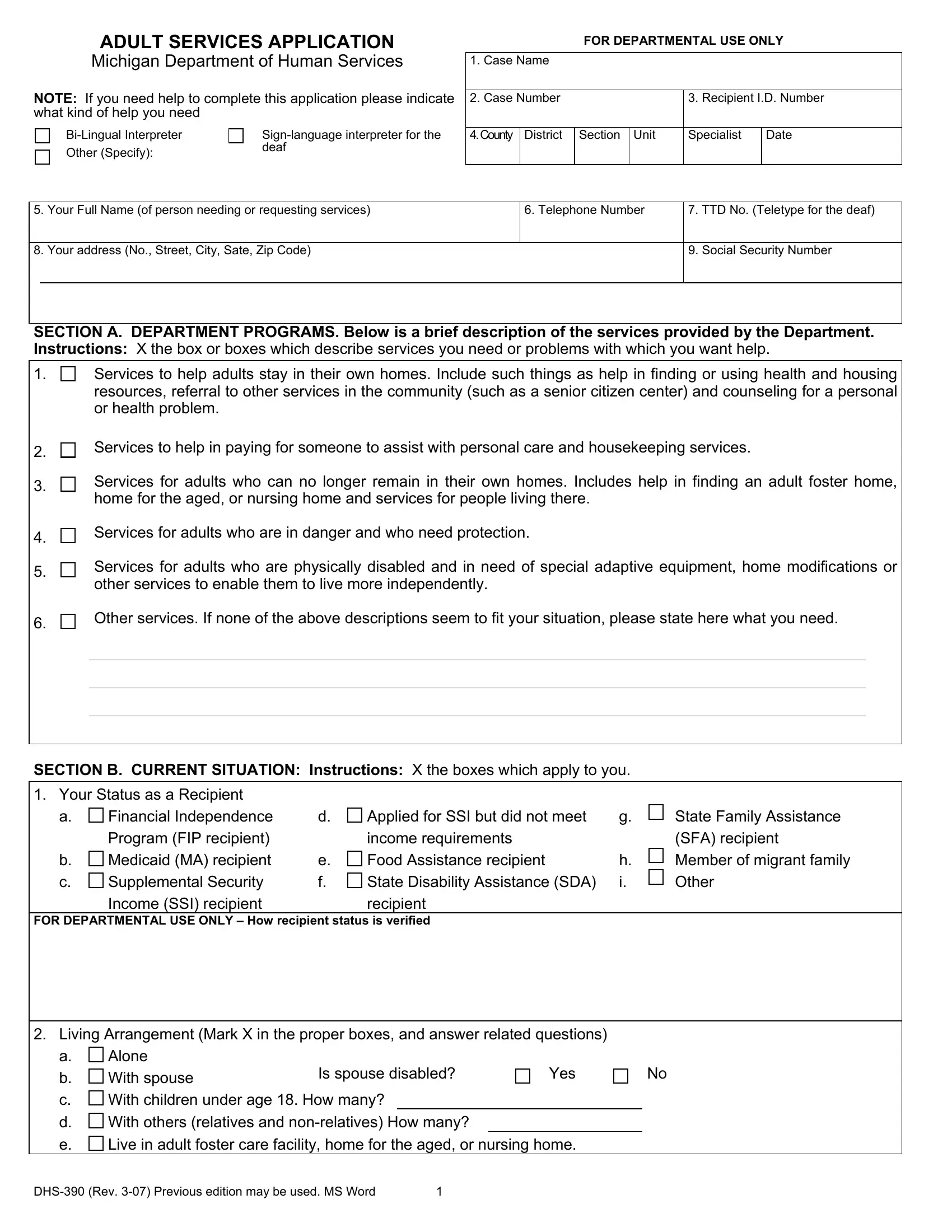
ADULT SERVICES APPLICATION
Michigan Department of Human Services
NOTE: If you need help to complete this application please indicate what kind of help you need
Other (Specify): |
deaf |
|
FOR DEPARTMENTAL USE ONLY
1. Case Name
2. Case Number |
3. Recipient I.D. Number |
||||
|
|
|
|
|
|
4.County |
District |
Section |
Unit |
Specialist |
Date |
|
|
|
|
|
|
5. |
Your Full Name (of person needing or requesting services) |
6. Telephone Number |
7. TTD No. (Teletype for the deaf) |
|
|
|
|
|
|
8. |
Your address (No., Street, City, Sate, Zip Code) |
|
9. Social Security Number |
|
|
|
|
|
|
|
|
|
|
|
SECTION A. DEPARTMENT PROGRAMS. Below is a brief description of the services provided by the Department. Instructions: X the box or boxes which describe services you need or problems with which you want help.
1. |
|
Services to help adults stay in their own homes. Include such things as help in finding or using health and housing |
||||||||
|
|
resources, referral to other services in the community (such as a senior citizen center) and counseling for a personal |
||||||||
|
|
or health problem. |
|
|
|
|
|
|
|
|
2. |
|
Services to help in paying for someone to assist with personal care and housekeeping services. |
||||||||
|
|
|
|
|
|
|
|
|
|
|
3. |
|
Services for adults who can no longer remain in their own homes. Includes help in finding an adult foster home, |
||||||||
|
home for the aged, or nursing home and services for people living there. |
|
|
|
||||||
|
|
|
|
|
||||||
4. |
|
Services for adults who are in danger and who need protection. |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
5. |
|
Services for adults who are physically disabled and in need of special adaptive equipment, home modifications or |
||||||||
|
other services to enable them to live more independently. |
|
|
|
|
|||||
|
|
|
|
|
|
|||||
6. |
|
Other services. If none of the above descriptions seem to fit your situation, please state here what you need. |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
|
|
|
||||||
SECTION B. CURRENT SITUATION: Instructions: X the boxes which apply to you. |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
1. |
Your Status as a Recipient |
|
|
|
|
|
|
|
|
|
|
a. |
Financial Independence |
d. |
Applied for SSI but did not meet |
g. |
State Family Assistance |
||||
|
|
Program (FIP recipient) |
|
income requirements |
|
|
(SFA) recipient |
|||
|
b. |
Medicaid (MA) recipient |
e. |
Food Assistance recipient |
|
h. |
Member of migrant family |
|||
|
c. |
Supplemental Security |
f. |
State Disability Assistance (SDA) |
i. |
Other |
||||
|
|
Income (SSI) recipient |
|
recipient |
|
|
|
|
||
FOR DEPARTMENTAL USE ONLY – How recipient status is verified |
|
|
|
|
||||||
|
|
|
|
|
|
|
||||
2. |
Living Arrangement (Mark X in the proper boxes, and answer related questions) |
|
|
|
||||||
|
a. |
Alone |
|
|
|
|
|
|
|
|
|
b. |
With spouse |
Is spouse disabled? |
Yes |
|
No |
||||
|
|
|
|
|
|
|
|
|
||
|
c. |
With children under age 18. How many? |
|
|
|
|
|
|||
|
d. |
With others (relatives and |
|
|
|
|
|
|||
|
e. |
Live in adult foster care facility, home for the aged, or nursing home. |
|
|
|
|||||
1 |
SECTION C. SERVICES APPLICATION RIGHTS, RESPONSIBLITIES AND INFORMATION: Instructions:
•Be sure to read this information. It describes your rights and responsibilities.
•You are entitled to a copy of this information.
•Ask for an explanation if you have questions.
1.You have the following rights:
APPLICATION – You have the right to apply for social services, to have your application reviewed with reasonable promptness, to be notified in writing of its approval or denial, and to be treated fairly and with dignity in all dealings with the department.
NONDISCRIMINATION – The Department of Human Services will not discriminate against any individual or group because of race, sex, religion, age, national origin, color, marital status, or handicap. If you believe you have been discriminated against you have a right to file a complaint with:
•Michigan Department of Human • Michigan Department of Civil • U.S. Department of Health and
Services |
Rights |
Human Services |
HEARINGS – If you believe that you have not been treated fairly or that a mistake has been made concerning your case, you have the right to appeal. This means that you will be given a right to request an appeal hearing by the Michigan Department of Community Health, at which time you will be able to explain your side to an impartial administrative law judge. Your right of appeal applies for any of the following reasons:
•The Department’s failure to act with reasonable promptness on your request for services.
•Any action by the Department which wrongly applies laws, rules or regulations to your particular situation.
•Any decision by the Department to refuse you services or to reduce or stop your services.
You may request a hearing in any other written form. You must sign and date a request for a hearing. You can send a request for a hearing to:
•Administrative Tribunal
Michigan Department of Community Health P.O. 30763
Lansing, MI 48909 FAX:
EXPLANATION ABOUT THE FOOD ASSISTANCE PROGRAM – If you do not currently receive food benefits, you have the right to be given the following information on the food assistance program:
•You may be eligible to receive food benefits.
•You may apply for the Food Assistance Program at your local Department of Human Services office.
VOTER REGISTRATION – If you are not registered to vote, you have the right to register.
2.You have the following responsibilities:
•To give full and correct information about your situation. Information you give may need to be verified.
•To report within 10 days to the Department of Human Services if your situation changes.
3.Read the following statement, sign and date the application.
•I WISH TO APPLY FOR SOCIAL SERVICES. I CERTIFY THAT THE INFORMATION I HAVE GIVEN IS CORRECT. I AGREE TO FULFILL THE RESPONSIBILITIES DESCRIBED IN THE RIGHTS, RESPONSIBILITIES AND INFORMATION SECTION ABOVE. IF YOU WISH FINANCIAL OR MEDICAL ASSISTANCE, ANOTHER APPLICATION IS NEEDED.
Signature of Client or Authorized Representative
Date
2 |