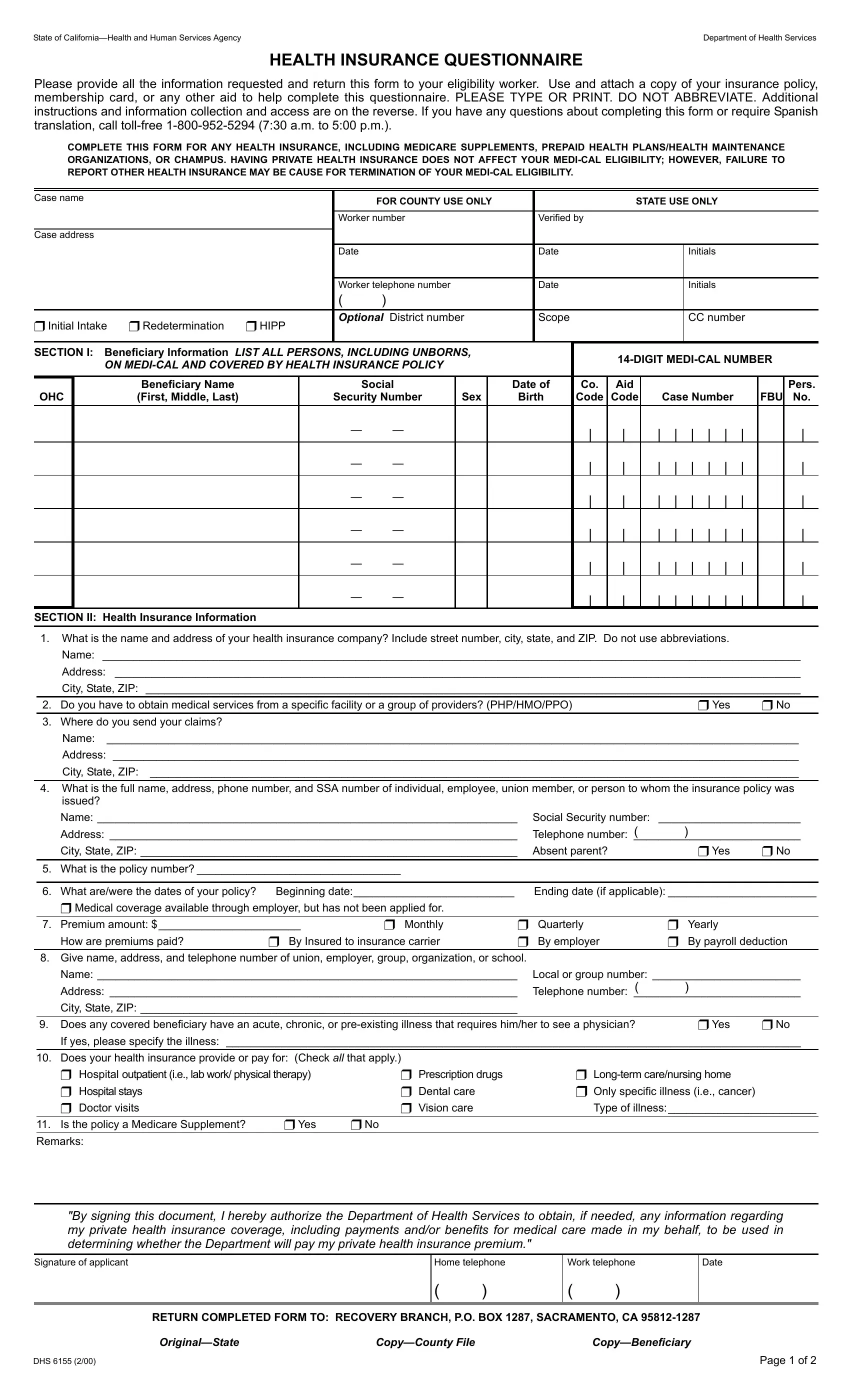
Navigating the complexities of healthcare benefits in California requires an understanding of various forms, one of which is the DHS 6155, a critical document for Medi-Cal beneficiaries. This Health Insurance Questionnaire mandates comprehensive details from applicants to ensure their eligibility for Medi-Cal benefits without being adversely affected by private health insurance plans they might also have. The form requires beneficiaries to disclose detailed personal and insurance policy information, emphasizing the necessity of reporting any other health insurance coverage as part of the eligibility evaluation process for Medi-Cal. It encompasses a range of inquiries from personal identification, such as social security numbers and Medi-Cal numbers, to health insurance specifics including policy numbers, types of coverage, and insurance providers' contact information. The document thoughtfully provides a section detailing the types of care covered by the insurance, including acute or chronic conditions, thus ensuring beneficiaries' medical needs are thoroughly assessed and addressed. Moreover, it explicitly states the requirement for Medi-Cal beneficiaries to assign rights to medical support or payments they are entitled to, from other sources, to the Medi-Cal program. This mechanism is designed to reimburse the program for expenses it covers that should have been billed to other health insurances, emblematic of Medi-Cal's role as the payer of last resort. Lastly, the form is equipped with instructions that affiliate closely with the Welfare and Institutions Code, highlighting the confidentiality of submitted information and the legal repercussions of non-disclosure, ultimately underscoring the significance of this form in the broader context of healthcare administration and patient care in California.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 6155 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | state of california health questionnaire, dhs 6155 form, dhs 6155 pdf, dhs 6155 |
State of |
Department of Health Services |
HEALTH INSURANCE QUESTIONNAIRE
Please provide all the information requested and return this form to your eligibility worker. Use and attach a copy of your insurance policy, membership card, or any other aid to help complete this questionnaire. PLEASE TYPE OR PRINT. DO NOT ABBREVIATE. Additional instructions and information collection and access are on the reverse. If you have any questions about completing this form or require Spanish translation, call
COMPLETE THIS FORM FOR ANY HEALTH INSURANCE, INCLUDING MEDICARE SUPPLEMENTS, PREPAID HEALTH PLANS/HEALTH MAINTENANCE ORGANIZATIONS, OR CHAMPUS. HAVING PRIVATE HEALTH INSURANCE DOES NOT AFFECT YOUR
Case name |
|
|
|
|
FOR COUNTY USE ONLY |
|
|
|
STATE USE ONLY |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Worker number |
|
|
|
Verified by |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Case address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
Date |
|
|
|
|
Initials |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Worker telephone number |
|
|
|
Date |
|
|
|
|
Initials |
|
|
|
|
||
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❼✶Initial Intake ❼✶Redetermination |
❼✶HIPP |
Optional District number |
|
Scope |
|
|
|
|
CC number |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SECTION I: |
Beneficiary Information LIST ALL PERSONS, INCLUDING UNBORNS, |
|
|
|
|
|||||||||||||||
|
|
ON |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Beneficiary Name |
|
|
Social |
|
|
Date of |
Co. |
Aid |
|
|
|
|
|
|
|
Pers. |
||
OHC |
|
(First, Middle, Last) |
|
|
Security Number |
Sex |
|
Birth |
Code |
Code |
|
Case Number |
|
FBU |
No. |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
— |
|
|
|
|
| |
| |
| |
| |
| |
| |
| |
| |
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
— |
— |
|
|
|
|
| |
| |
| |
| |
| |
| |
| |
| |
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
— |
— |
|
|
|
|
| |
| |
| |
| |
| |
| |
| |
| |
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
— |
— |
|
|
|
|
| |
| |
| |
| |
| |
| |
| |
| |
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
— |
— |
|
|
|
|
| |
| |
| |
| |
| |
| |
| |
| |
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
— |
— |
|
|
|
|
| |
| |
| |
| |
| |
| |
| |
| |
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
SECTION II: Health Insurance Information
1.What is the name and address of your health insurance company? Include street number, city, state, and ZIP. Do not use abbreviations.
Name: _________________________________________________________________________________________________________________
Address: _______________________________________________________________________________________________________________
City, State, ZIP: __________________________________________________________________________________________________________
2. |
Do you have to obtain medical services from a specific facility or a group of providers? (PHP/HMO/PPO) |
❼ Yes |
❼ No |
3. |
Where do you send your claims? |
|
|
Name: ________________________________________________________________________________________________________________
Address: _______________________________________________________________________________________________________________
City, State, ZIP: _________________________________________________________________________________________________________
4.What is the full name, address, phone number, and SSA number of individual, employee, union member, or person to whom the insurance policy was issued?
|
Name: ____________________________________________________________________ |
Social Security number: |
_______________________ |
||
|
Address: __________________________________________________________________ |
( |
) |
|
|
|
Telephone number: ___________________________ |
||||
|
City, State, ZIP: _____________________________________________________________ |
Absent parent? |
❼ Yes |
❼ No |
|
|
|
|
|
|
|
5. |
What is the policy number? _________________________________ |
|
|
|
|
|
|
|
|
||
6. |
What are/were the dates of your policy? |
Beginning date:__________________________ |
Ending date (if applicable): ________________________ |
||
❼Medical coverage available through employer, but has not been applied for.
7. |
Premium amount: $_______________________ |
❼ Monthly |
❼ Quarterly |
❼ Yearly |
|
||||
|
|
How are premiums paid? |
❼ By Insured to insurance carrier |
❼ By employer |
❼ By payroll deduction |
||||
|
|
|
|
|
|||||
8. |
Give name, address, and telephone number of union, employer, group, organization, or school. |
|
|
||||||
|
|
Name: ____________________________________________________________________ |
Local or group number: ________________________ |
||||||
|
|
Address: __________________________________________________________________ |
( |
) |
|
||||
|
|
Telephone number: ___________________________ |
|||||||
|
|
City, State, ZIP: _____________________________________________________________ |
|
|
|
||||
|
|
|
|
|
|||||
9. |
Does any covered beneficiary have an acute, chronic, or |
❼ Yes |
❼ No |
||||||
|
|
If yes, please specify the illness: _____________________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|||
10. |
Does your health insurance provide or pay for: (Check all that apply.) |
|
|
|
|
||||
|
|
❼ |
Hospital outpatient (i.e., lab work/ physical therapy) |
❼ |
Prescription drugs |
❼ |
|
||
|
|
❼ |
Hospital stays |
|
❼ |
Dental care |
❼ Only specific illness (i.e., cancer) |
|
|
|
|
❼ |
Doctor visits |
|
❼ |
Vision care |
Type of illness:________________________ |
||
|
|
|
|
|
|
|
|
|
|
11. |
Is the policy a Medicare Supplement? |
❼ Yes |
❼ No |
|
|
|
|
||
Remarks:
"By signing this document, I hereby authorize the Department of Health Services to obtain, if needed, any information regarding my private health insurance coverage, including payments and/or benefits for medical care made in my behalf, to be used in determining whether the Department will pay my private health insurance premium."
Signature of applicant
Home telephone
()
Work telephone
()
Date
RETURN COMPLETED FORM TO: RECOVERY BRANCH, P.O. BOX 1287, SACRAMENTO, CA
DHS 6155 (2/00) |
|
Page 1 of 2 |

INSTRUCTIONS
Section I: Beneficiary Information
List the names (first, middle, last) of all persons on
Section II: Health Insurance Information
Item No. 1: Enter the full name and mailing address of your insurance company. (Include street address and/or P.O. Box, city, state, and ZIP.) DO NOT USE ABBREVIATIONS!
Item No. 2: Check the appropriate box if you have to obtain medical services from a specific facility or a group of providers (Prepaid health plans [PHP], Health Maintenance Organizations [HMO], Preferred Providers Organizations [PPO]).
Item No. 3: Enter the complete name and mailing address where your health insurance claims are sent. Only complete if different from the answer to Item No.1.
Item No. 4: Enter the full name, mailing address, telephone number, and Social Security number of the individual, employee, union member, retired employee, or person to whom the insurance policy is or was issued (insured). Check the appropriate box for an absent parent.
Item No. 5: Enter the number the insurance company needs to identify the policy. This number is sometimes called: subscriber, certificate, account, employee, group, and local number.
Item No. 6: Enter the date (month/day/year) the insurance policy began and date terminated. If known, enter the policy lapse dates, and check the box if medical coverage is available through an employer which has not been applied for.
Item No. 7: Enter the premium amount; check the box if they are paid per month, quarter, or year, and how the premiums are paid. Check appropriate box(es).
Item No. 8: If the policy is purchased through a union, employer, group, organization, or school, enter the name, address, telephone number, local or group number, if known.
Item No. 9: Check the box "YES" or "NO" if any covered beneficiary has an acute or chronic
Item No. 10: Read and check items which apply to your insurance coverage.
Item No. 11: Read and check yes or no.
Signature Section: Please sign the form and give your home and/or work telephone number. If you do not have a telephone, please put a message number in the home telephone box. Also, enter the date when you completed this form.
IMPORTANT: As a condition of eligibility, all
INFORMATION COLLECTION AND ACCESS
Sections 50761 and 50763 of Title 22, California Code of Regulations (CCR), requires recipients to report other health coverage to which they are entitled.
The information requested is necessary to make possible the recovery of health insurance or other contractual or legal entitlements as provided in Welfare and Institutions Code, Sections 10020 through 10025, 14024, 14103, and 14124.70, from persons liable thereunder.
Information concerning your health coverage is maintained by the Chief of the Recovery Branch, by authority of the Welfare and Institutions Code, Section 14011, and Title 22, California Code of Regulations, Section 50769. All information is mandatory.
Section 14023 of the Welfare and Institutions Code provides that any public assistance recipient who has any other contractual or legal entitlement to any health care service and who willfully refuses to disclose this information by withholding important information regarding other medical entitlement is guilty of a misdemeanor.
DHS 6155 (2/00) |
Page 2 of 2 |