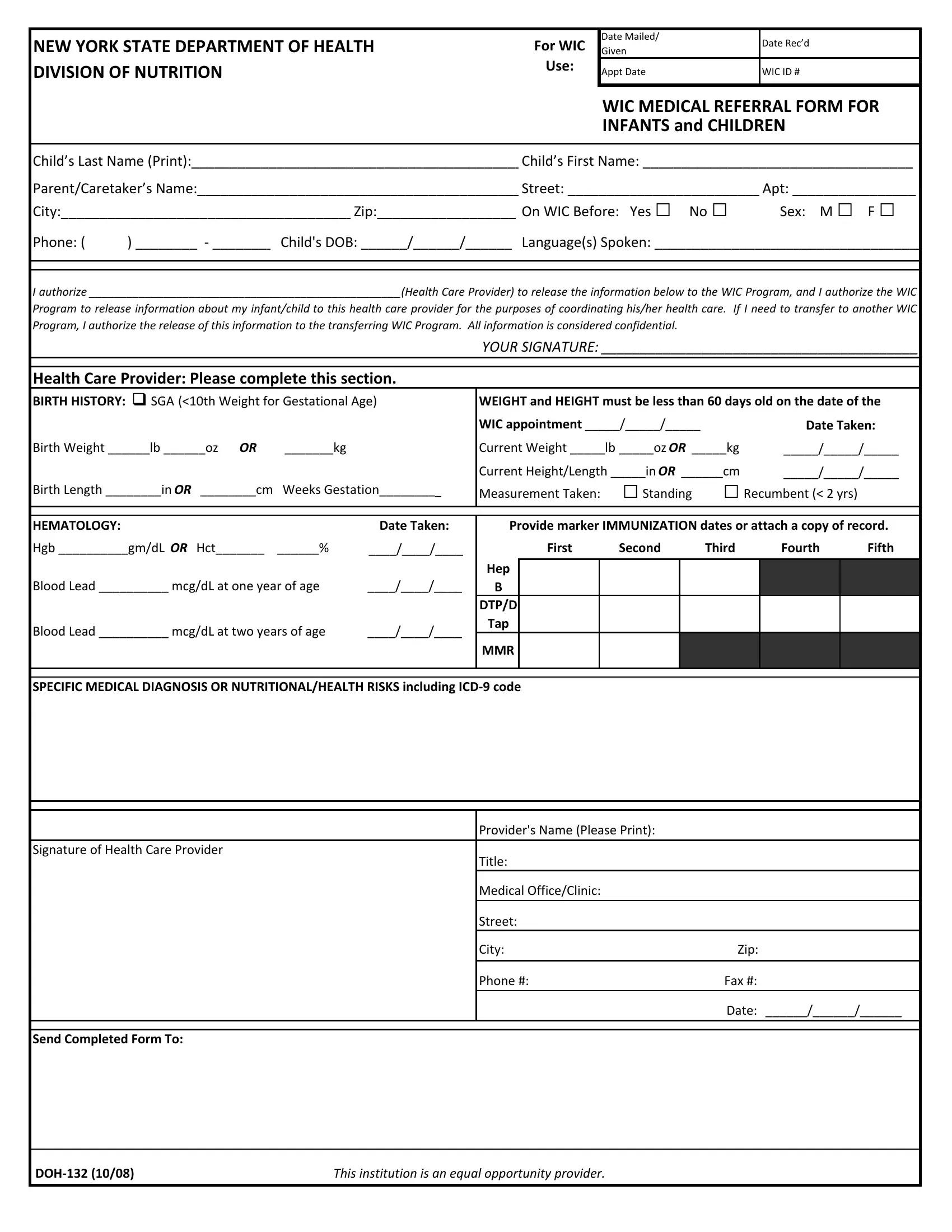
In order to file for a divorce in the state of Ohio, you must complete and submit Form Doh 132. This form is used to provide information about both you and your spouse, as well as the reasons for your divorce. It's important to complete this form accurately and completely, in order to ensure that your divorce process goes as smoothly as possible. If you have any questions about completing Form Doh 132, be sure to consult an attorney.
| Question | Answer |
|---|---|
| Form Name | Doh 132 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wic nyc pdf, Recumbent, MMR, Hct |
NEW YORK STATE DEPARTMENT OF HEALTH |
For WIC |
Date Mailed/ |
Date Rec’d |
|
Given |
||||
|
||||
DIVISION OF NUTRITION |
Use: |
Appt Date |
WIC ID # |
|
|
||||
|
|
|
|
WIC MEDICAL REFERRAL FORM FOR
INFANTS and CHILDREN
Child’s Last Name (Print):___________________________________________ Child’s First Name: ___________________________________
Parent/Caretaker’s Name:__________________________________________ Street: _________________________ Apt: ________________ |
||||
City:______________________________________ Zip:__________________ On WIC Before: Yes □ |
No □ |
Sex: M □ |
F □ |
|
Phone: ( |
) ________ ‐ ________ Child's DOB: ______/______/______ Language(s) Spoken: ___________________________________ |
|||
I authorize __________________________________________________(Health Care Provider) to release the information below to the WIC Program, and I authorize the WIC
Program to release information about my infant/child to this health care provider for the purposes of coordinating his/her health care. If I need to transfer to another WIC Program, I authorize the release of this information to the transferring WIC Program. All information is considered confidential.
YOUR SIGNATURE: _________________________________________
Health Care Provider: Please complete this section.
BIRTH HISTORY: |
SGA (<10th Weight for Gestational Age) |
WEIGHT and HEIGHT must be less than 60 days old on the date of the |
||||||||||
|
|
|
|
WIC appointment _____/_____/_____ |
|
Date Taken: |
||||||
Birth Weight ______lb ______oz OR |
_______kg |
Current Weight _____lb _____oz OR _____kg |
_____/_____/_____ |
|||||||||
|
|
|
|
Current Height/Length _____in OR ______cm |
_____/_____/_____ |
|||||||
Birth Length ________in OR ________cm |
Weeks Gestation_________ |
Measurement Taken: |
□Standing |
□Recumbent (< 2 yrs) |
|
|||||||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|||
HEMATOLOGY: |
|
|
Date Taken: |
Provide marker IMMUNIZATION dates or attach a copy of record. |
||||||||
Hgb __________gm/dL OR Hct_______ |
______% |
____/____/____ |
|
First |
Second |
Third |
Fourth |
Fifth |
||||
|
|
|
|
Hep |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood Lead __________ mcg/dL at one year of age |
____/____/____ |
B |
|
|
|
|
|
|
|
|
||
|
|
|
|
DTP/D |
|
|
|
|
|
|
|
|
Blood Lead __________ mcg/dL at two years of age |
____/____/____ |
Tap |
|
|
|
|
|
|
|
|
||
MMR |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
||||||
SPECIFIC MEDICAL DIAGNOSIS OR NUTRITIONAL/HEALTH RISKS including ICD‐9 code |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider's Name (Please Print): |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Health Care Provider |
|
|
Title: |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Medical Office/Clinic: |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Street: |
|
|
|
|
|
|
||
|
|
|
|
City: |
|
|
Zip: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Phone #: |
|
|
Fax #: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Date: ______/______/______ |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Send Completed Form To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
DOH‐132 (10/08) |
|
|
This institution is an equal opportunity provider. |
|
|
|
|
|
|
|||