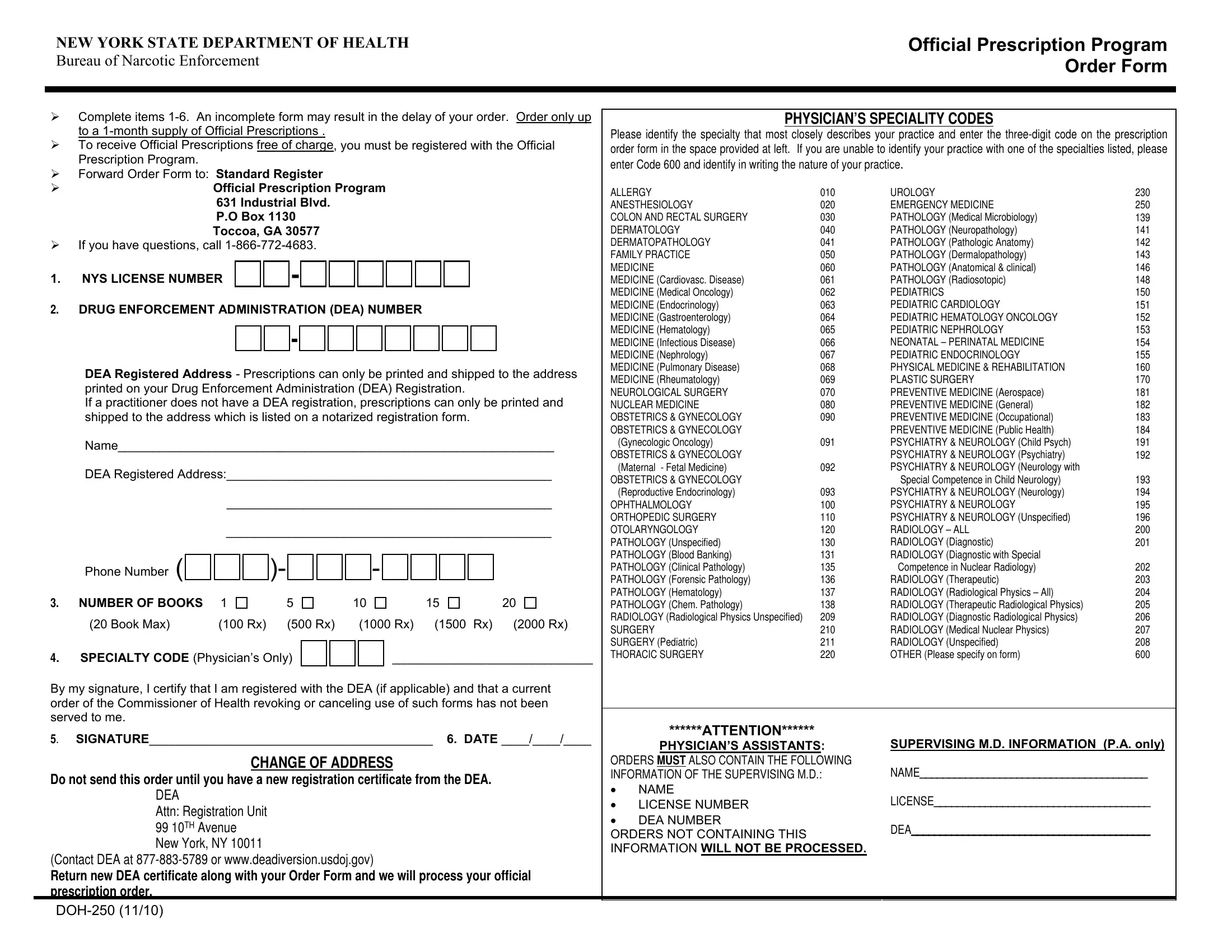
The New York State Department of Health Official Prescription Program plays a pivotal role in the regulation and distribution of official prescriptions through its comprehensive Order Form, DOH-250. This form is intricately designed to streamline the ordering process for up to a one-month supply of official prescriptions, ensuring that healthcare practitioners maintain an adequate stock for their practice needs while adhering to stringent regulatory standards. To facilitate this, the form requires detailed information spanning from the practitioner's New York State license number and Drug Enforcement Administration (DEA) number to a specific physician's specialty code—an essential component that identifies the nature of the practice with impressive granularity. With a meticulous list of specialties including everything from Allergy to Urology, and even accommodating practices that may not fit neatly into predefined categories with a "600" code option, it underscores the form's adaptability. The submission process demands thoroughness; any gaps in information can delay the order, emphasizing the bureaucratic precision required in controlled substance management. This form also caters to specific scenarios, such as changes in address, by necessitating the updated registration information—a demonstration of the program’s commitment to ensuring that prescriptions are only printed and shipped to verified addresses. Moreover, the allowance for a range of ordered books reflects a tailored approach to practitioners' varying needs, supported further by guidance for physician assistants overseeing MD information, underscoring the comprehensive nature of the DOH-250 form in maintaining the integrity and efficiency of prescription distribution within the healthcare sector.
| Question | Answer |
|---|---|
| Form Name | Form Doh 250 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Rx, deadiversion, Radiosotopic, New_York |

|
NEW YORK STATE DEPARTMENT OF HEALTH |
|
|
|
|
|
|
|
Official Prescription Program |
||||||||||||||||||||||||||
|
BUREAU OF NARCOTIC ENFORCEMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Order Form |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Complete items |
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
PHYSICIAN’S SPECIALITY CODES |
|
|||||||||||||||||||||||||||||||
|
|
to a |
|
|
|
|
|
|
|
|
|
|
|
|
|
Please identify the specialty that most closely describes your practice and enter the |
|||||||||||||||||||
|
|
To receive Official Prescriptions free of charge, you must be registered with the Official |
|||||||||||||||||||||||||||||||||
|
|
order form in the space provided at left. If you are unable to identify your practice with one of the specialties listed, please |
|||||||||||||||||||||||||||||||||
|
|
Prescription Program. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
enter Code 600 and identify in writing the nature of your practice. |
|
|||||
|
|
Forward Order Form to: Standard Register |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
Official Prescription Program |
|
|
|
|
ALLERGY |
010 |
UROLOGY |
230 |
|||||||||||||||||||||||
|
|
|
|
|
631 Industrial Blvd. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANESTHESIOLOGY |
020 |
EMERGENCY MEDICINE |
250 |
||||||||||||||
|
|
|
|
|
P.O Box 1130 |
|
|
|
|
|
|
|
|
|
|
|
|
|
COLON AND RECTAL SURGERY |
030 |
PATHOLOGY (Medical Microbiology) |
139 |
|||||||||||||
|
|
|
|
Toccoa, GA 30577 |
|
|
|
|
|
|
|
|
|
|
|
|
|
DERMATOLOGY |
040 |
PATHOLOGY (Neuropathology) |
141 |
||||||||||||||
|
|
If you have questions, call |
|
|
|
|
|
|
|
|
|
|
|
|
|
DERMATOPATHOLOGY |
041 |
PATHOLOGY (Pathologic Anatomy) |
142 |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FAMILY PRACTICE |
050 |
PATHOLOGY (Dermalopathology) |
143 |
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICINE |
060 |
PATHOLOGY (Anatomical & clinical) |
146 |
|
1. |
NYS LICENSE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICINE (Cardiovasc. Disease) |
061 |
PATHOLOGY (Radiosotopic) |
148 |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICINE (Medical Oncology) |
062 |
PEDIATRICS |
150 |
|
2. |
DRUG ENFORCEMENT ADMINISTRATION (DEA) NUMBER |
|
|
|
|
MEDICINE (Endocrinology) |
063 |
PEDIATRIC CARDIOLOGY |
151 |
||||||||||||||||||||||||||
|
|
|
|
MEDICINE (Gastroenterology) |
064 |
PEDIATRIC HEMATOLOGY ONCOLOGY |
152 |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICINE (Hematology) |
065 |
PEDIATRIC NEPHROLOGY |
153 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICINE (Infectious Disease) |
066 |
NEONATAL – PERINATAL MEDICINE |
154 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICINE (Nephrology) |
067 |
PEDIATRIC ENDOCRINOLOGY |
155 |
|
|
|
DEA Registered Address - Prescriptions can only be printed and shipped to the address |
MEDICINE (Pulmonary Disease) |
068 |
PHYSICAL MEDICINE & REHABILITATION |
160 |
|||||||||||||||||||||||||||||
|
|
MEDICINE (Rheumatology) |
069 |
PLASTIC SURGERY |
170 |
||||||||||||||||||||||||||||||
|
|
printed on your Drug Enforcement Administration (DEA) Registration. |
|
||||||||||||||||||||||||||||||||
|
|
|
NEUROLOGICAL SURGERY |
070 |
PREVENTIVE MEDICINE (Aerospace) |
181 |
|||||||||||||||||||||||||||||
|
|
If a practitioner does not have a DEA registration, prescriptions can only be printed and |
|||||||||||||||||||||||||||||||||
|
|
NUCLEAR MEDICINE |
080 |
PREVENTIVE MEDICINE (General) |
182 |
||||||||||||||||||||||||||||||
|
|
shipped to the address which is listed on a notarized registration form. |
|
OBSTETRICS & GYNECOLOGY |
090 |
PREVENTIVE MEDICINE (Occupational) |
183 |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OBSTETRICS & GYNECOLOGY |
|
PREVENTIVE MEDICINE (Public Health) |
184 |
|
|
|
Name_______________________________________________________________ |
|
(Gynecologic Oncology) |
091 |
PSYCHIATRY & NEUROLOGY (Child Psych) |
191 |
||||||||||||||||||||||||||||
|
|
OBSTETRICS & GYNECOLOGY |
|
PSYCHIATRY & NEUROLOGY (Psychiatry) |
192 |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
DEA Registered Address:_______________________________________________ |
|
(Maternal - Fetal Medicine) |
092 |
PSYCHIATRY & NEUROLOGY (Neurology with |
|
||||||||||||||||||||||||||||
|
|
OBSTETRICS & GYNECOLOGY |
|
Special Competence in Child Neurology) |
193 |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
_______________________________________________ |
|
(Reproductive Endocrinology) |
093 |
PSYCHIATRY & NEUROLOGY (Neurology) |
194 |
||||||||||||||||||||||||||
|
|
|
|
OPHTHALMOLOGY |
100 |
PSYCHIATRY & NEUROLOGY |
195 |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ORTHOPEDIC SURGERY |
110 |
PSYCHIATRY & NEUROLOGY (Unspecified) |
196 |
|
|
|
|
|
_______________________________________________ |
OTOLARYNGOLOGY |
120 |
RADIOLOGY – ALL |
200 |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATHOLOGY (Unspecified) |
130 |
RADIOLOGY (Diagnostic) |
201 |
|
|
|
Phone Number ( |
|
|
|
|
|
|
|
|
)- |
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
PATHOLOGY (Blood Banking) |
131 |
RADIOLOGY (Diagnostic with Special |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATHOLOGY (Clinical Pathology) |
135 |
Competence in Nuclear Radiology) |
202 |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATHOLOGY (Forensic Pathology) |
136 |
RADIOLOGY (Therapeutic) |
203 |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
3. |
NUMBER OF BOOKS |
1 |
|
|
|
|
|
5 |
|
|
|
|
|
10 |
|
|
|
|
|
|
15 |
|
|
20 |
PATHOLOGY (Hematology) |
137 |
RADIOLOGY (Radiological Physics – All) |
204 |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATHOLOGY (Chem. Pathology) |
138 |
RADIOLOGY (Therapeutic Radiological Physics) |
205 |
||||||||||||||
|
|
(20 Book Max) |
|
(100 Rx) |
(500 Rx) |
|
|
(1000 Rx) |
(1500 Rx) |
(2000 Rx) |
RADIOLOGY (Radiological Physics Unspecified) |
209 |
RADIOLOGY (Diagnostic Radiological Physics) |
206 |
|||||||||||||||||||||
|
|
|
|
|
SURGERY |
210 |
RADIOLOGY (Medical Nuclear Physics) |
207 |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SURGERY (Pediatric) |
211 |
RADIOLOGY (Unspecified) |
208 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
4. |
SPECIALTY CODE (Physician’s Only) |
|
|
|
|
|
_____________________________ |
THORACIC SURGERY |
220 |
OTHER (Please specify on form) |
600 |
||||||||||||||||||||||||
|
By my signature, I certify that I am registered with the DEA (if applicable) and that a current |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
order of the Commissioner of Health revoking or canceling use of such forms has not been |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
served to me. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
5. |
SIGNATURE_________________________________________ 6. DATE ____/____/____ |
|
******ATTENTION****** |
|
|
|
|||||||||||||||||||||||||||||
|
PHYSICIAN’S ASSISTANTS: |
SUPERVISING M.D. INFORMATION (P.A. only) |
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
CHANGE OF ADDRESS |
|
|
|
|
ORDERS MUST ALSO CONTAIN THE FOLLOWING |
NAME________________________________________ |
|||||||||||||||||||||
|
Do not send this order until you have a new registration certificate from the DEA. |
|
INFORMATION OF THE SUPERVISING M.D.: |
||||||||||||||||||||||||||||||||
|
|
• |
NAME |
|
|
|
|||||||||||||||||||||||||||||
|
|
DEA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE______________________________________ |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• |
LICENSE NUMBER |
|
||||
|
|
Attn: Registration Unit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• |
DEA NUMBER |
|
|
|
|||||||||
|
|
99 10TH Avenue |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEA__________________________________________ |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ORDERS NOT CONTAINING THIS |
|
||||||||||||
|
|
New York, NY 10011 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFORMATION WILL NOT BE PROCESSED. |
|
|
|||||||||||
|
(Contact DEA at |
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
Return new DEA certificate along with your Order Form and we will process your official |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
prescription order. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||